10. Lower GI Pathology Flashcards
(14 cards)
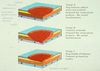
What pathologies do these 3 images show?

Top L: colorectal polyps; Top R: colorectal carcinoma (central, pitting + polyps); Bottom L: IBD - cobblestoning = advanced CD/UC, wall thickened = more often assocaited wtih CD
Describe the 4 types of polyp.
How might someone with colonic polyps present?
Inflammatory: e.g. UC and CD. Granular and rough - lots of inflammtory cells. Can arise at site of previous anastamosis, or from ischaemia
Hyperplastic: common, usually asymptomatic, benign. Pale, flat lesions up to 5mm - mucosa has trouble shedding its most superfifical layer. 50-80% in rectosigmoid
Harmartomatous: uncommon, children and young adults, Peutz-Jeghers’ (autosomal dominant) and juvenile polyps are commonest. Recapitulation of normal tissue - more glands, SM hyperplasia
Neoplastic (adenomas): common, incidence increases with age, sporadic but can be familial. Premalignant condition
Rectal bleeding, most commonly encountered by chance
What are the 4 types of neoplastic polyp (adenoma)?
What are these types of adenomas? [pic]
What is the adenoma-carcinoma sequence?

Tubular, villous, tubovillous, serrated (assocaited with increased risk in colorectal cancer)
- *L: tubular adenoma** - can see pedunculated polyp with stalk. If <1cm, lower risk of adenocarcinoma. Darker parts on histology = abnormal proliferating glands
- *R: villous adenoma** - follow up pt more aggressively e.g. colonoscopy in 3 years. Degree of dysplasia important
Most colorectal carcinomas arise within a pre-existing adenoma [Pic]

What is the epidemiology of colorectal cancer (% of UK cancers, M:F etc.)?
What are some high and low incidence areas?
What are some predisposing factors?
Where are the most common sites for colorectal cancers?
15% of all cancer deaths in UK. Peak incidence 60-70 years (if <40, start screening family). M>F. USUALLY ADENOCARCINOMA
High: USA, canada, UK, denmark. Mostly L-sided tumours
Low: colombia, Japan, india, south africa. Mostly R-sided tumours
Neoplastic polyps, adenomas, polyposis syndromes e.g. Peutz-Jeghers’, IBD, genetics, diet (low fibre, high red meat), smoking, alcohol, urban environment
Rectosigmoid (75%); Descending & transverse (30%); Proximal (15%)
List the presenting features for rectosigmoid (left sided) tumours and right sided tumours.
What is the macroscopic appearance of colonic cancer?
What are the microscopic features?
Left sided: change in bowel habit, rectal bleeding, obstruction
Right sided: anaemia (Hb decrease), anorexia/wt loss, abdominal pain, obstruction less likely
Polypoid fungating (protude into lumen) [L pic = polypoid mass], uncerating (into mucosa), annular constructing (forms stricture) [R pic], diffuse infiltrating (subtle to detect)
Adenocarcinoma (95%, arise from glandular epithelium, bottom pic, see increased nuclear:cytoplasm, enlarged nuceli, increased mitotic activity), undifferentiated carcinoma (5%)

What are the ways colonic carcinoma can spread?
Describe the 2 ways of staging these cancers.
Direct/local, lymphatic, haematogenous (into BVs), transcoelomic (across peritoneum/body cavity)
- *Dukes’: stages A-D:** [pic]
- *A -** limited to muscularis mucosae
- *B -** extension through muscularis mucosae
- *C-** involement of regional LN
- *D -** distant metastasis
- *TNM:** (most commonly used):
- *Tx:** primary tumour can’t be assessed
- *Tis:** carcinoma in situ (group of abnormal cells)
- *T0:** no evidence of primary tumour
- *T1:** confined to lamina propria
- *T2:** within bowel wall
- *T3:** through bowel wall into serosa
- *T4:** up to serosal surface
- *N0:** no node involement
- *N1:** 1-3 nodes involeved
- *N2:** 4 or more nodes involved
- *M0:** no distant spread
- *M1:** distant metastases
Describe the screening programme for colorectal cancer.
What does IBD cover?
Briefly describe the 2 types of idiopathic IBD.
National programme, when age 60-74, every 2 years, FOB (faecal occult blood) +/- colonoscopy. Aim = detect adenomas
Ulcerative colitis, Crohn’s disease, infective colitis (e.g. C. diff colitis), ischaemic colitis (assocaited with PAD), pseudomembraneous colitis, radiation colitis (e.g cervical cancer hx), microscopic colitis (lymphocytic or collagenous), drug-induced colitis (e.g. amphetamines)
1. Ulcerative Colitis: relapsing and remitting, inflammation limited to mucosa, involves large bowel only
2. Crohn’s disease: recurrent granulomatous disease, transmural inflammation, affects any part of ailementary tract
Compare the epidemiology of ulcerative colitis and Crohn’s disease.
Compare the distribution of ulcerative colitis and Crohn’s disease.
UC: relatively common, any age (20-40yrs), M:F = 2:3, worldwide
CD: less common, any age (20-30yrs), M:F = 1:1, high and low incidence countries
UC: begins in rectum, spreads proximally in continuity, terminal ileum involved in 10% of cases of total colitis (“backwash ileitis”). May effect just rectum (proctitis ~50%), involve part of the colon (L-sided colitis ~30%), or entire colon (pancolitis ~20%)
CD: any part of alimentary tract involved (terminal ileum 80%, anus 25%), lesions discontinuous (skip lesions)
Compare the presenting features of ulcerative colitis and Crohn’s disease.
Compare the macroscopic features of ulcerative colitis and Crohn’s disease.
UC: bloody diarrhoea, abdo pain
Crohn’s: bloody diarrhoea, abdo pain, anorexia/wt loss, perianal disease, growth failure
UC: active phase = red mucosa, friable, granular, oedematous; quiescent phase: mucosa atrophic and featureless. NB after tx may see skip lesions as it heals - not CD!
CD: affected bowel wall (thickened, rigid (hosepipe thickening), narrowed lumen), affected serosa (granula, fibrotic, fat “wrapping”), affected mucosa (aphthoid, fissuring and serpinginous ulcers, cobblestoning)
Identify the pathologies in A-G

a) acute ulcerative colitis
b) cobblestoning (CD)
c) fat wrapping (CD)
d) hosepipe thickening (CD)
e) apthous lesions (CD, also see lots of neutrophils)
f) perianal fistulae
g) skip lesions (CD)
What are some microscopic features of ulcerative colitis and Crohn’s disease?
What do the following histologies show?

UC: mucosal disease only: normal submucosa and muscularis propria, inflamed mucosa
CD: transmural disease, granulomas. See lymphoid aggregates all the way through the different layers
Top L: UC - inflamed mucosa only. Top R: CD - transmural inflammation.
Bottom: CD - granulomas (granulomas in TB as well - follow up!)
What are some local complications of ulcerative colitis and Crohn’s?
What does the image show, and what is it more commonly seen in (UC or CD)?
What are some systemic complications of UC and CD?

UC: acute fulminant colitis (acute dilation of tranverse colon -> extensive ulceration, transmural inflammation and perforation), malignant change
CD: strictures (-> obstruction), fistula formation (between bowel and abdominal viscera), malabsorption, perianal disease
Toxic megacolon - complication of IBD, most commonly UC. Acute toxic colitis + colon distension. See abdo distension, sometimes fever, shock or abdo pain. Can see multiple scarring from fistula. Protruding red = fistula
UC: Skin - erythema nodosum, pyoderma gangrenosum. Joints - seronegative polyarthritis. Eye - iritis, episcleritis. Kidney - calculi (stones), pyelonephritis. Liver - sclerosing cholangitis (chronic liver disease)
CD: Skin - erythema nodosum, pyoderma gangrenosum. Joints - seronegative polyarthritis. Eye - iritis, episcleritis. Kidney - calculi, pyelonephrits. Amyloidosis
What pathologies do the two images show?
What is the aetiology/pathogenesis of IBD?
Are (colorectal) carcinomas more likely in ulcerative colitis or Crohn’s disease?

L: erythema nodosum - painful, hard leg nodules; R: pyoderma gangrenosum - very inflamed
Genetic factors (higher risk if 1st degree relative with IBD), environmental, micro-organisms, immunological factors, other theories…
UC
What factors does the risk of carcinoma in ulcerative colitis vary according to?
What is identification and prognosis like for carcinomas in ulcerative colitis?
Disease extent, duration and age of onset of colitis. (Longer = more likely to develop cancer)
Often flat and difficult to visualise (due to dysplasia), often poorly differentiated. Prognosis poor due to late presentation.
