11 - Pharmacokinetics Drug In Flashcards
(31 cards)
What is pharmacokinetics?
What the body does to the drug
What is
- Pharmaceutical process?
- Pharmacokinetic process?
- Pharmacodynamic process?
- Therapeutic process?
- Is the drug getting into the patient
- Is the drug getting to the site of action
- Is drug producing the desired effect
- Is this translated to a therapeutic effect
What are the main factors affecting rate of drug in and drug out?
- Absorption
- Distribution
- Metabolism
- Excretion
What are the different sites of administration of drugs?

What are the advantages of focal administration?
- Concentrates drug at site
- Prevents side effects
e. g local steroids
What are the different ways of administering a drug orally?
- Tablet (rate of action depends on rate of dissolution)
- Liquid (faster)
BEST WAY TO ADMINISTER DRUGS IS ORALLY
How do drugs get absorbed via the enteral route?
SI: 6-7m length, 2.5 diameter

What ways can drugs be absorbed when they are in the body?
- Passive Diffusion (lipophilic uncharged)
- Facilitated Diffusion
- Pinocytosis
- Primary/Secondary active transport
What is valproate and how is it absorbed?
- Antiepileptic drug
- pKa = 5 so slightly protonated (10%)
- Lipophilic so absorbed
- As long transit time more chance to become protonated and absorbed

How are charged drugs absorbed by faciltated diffusion?
Solute carrier family (SLC) (OCT and OAT’s)
What are the properties of SLC’s?
- Large family
- Important for drug absorption and elimination
- Larged expressed in GI, renal and hepatic epithelia
What drugs are absorbed by SLC secondary active transport?
- Prozac: antidepressant co-transported with Na+
- Penicillin: antibiotic co-transported with H+
What factors affect drug absorption?

Give examples of a drug absorbed by OAT and OCT?
OCT - Metformin (diabetes)
OAT - Methotrexate (cancer)
What is first pass metabolism?
Concentration of a drug is largely reduced before it reaches systemic circulation

How do you avoid first pass metabolism?
- Different route of administration if large concentration of drug lost e.g parenteral, rectal, sublingual (glyceryl trinitrate)
What is oral bioavailability of a drug?
Proportion of drug given orally that reaches the systemic circulation unchanged
Measured by amount and rate
How do you calculate oral bioavailability and what does this determine?
Determines route of administration

What factors affect drug distribution?
- Drug lipophilicity
- Capillary permeability
- OAT/OLC Expression
- Drug pKa and local pH
- Drug binding to proteins and lipids (albumin and LDL)
What is the importance of drugs binding to plasma proteins?
- Bind in equillibrium
- Only free drug can bind to receptors
- Protein bound drug acts as a reservoir
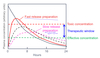
What is therapeutic index?
- Got to keep drug concentration between therapeutic window
(Median Lethal Dose/Median Effective Dose)

What is the volume of distribution?
- Theoretical volume into which drug is distributed if this occurred instantaneously
- Extrapolate back to zero

Why do you need to look at the therapeutic ratio when deciding what concentration to give for different administation purposes?
If fast release preparation was same concentration of slow release preparation then the dose may go over the therapeutic window
How do you interpret the volume of distribution and what are the units?
- Small Vd, lots in blood, little distribution
- Large Vd, little in blood, lots of distribution
- Litres or L/Kg (standard)


