4.2-Gastric & Peptic Ulcer Disease Flashcards
(32 cards)
What are the normal secretory components of the stomach?
- Upper 2/3s; parietal cells secrete HCl and intrinsic factor and chief cells secrete pepsinogen
- Lower 1/3 secretes bicarbonate-rich mucus (mucus cells)+ gastrin from G cels
Name some common symptoms of gastritis and PUD?
- dyspepsia
- anorexia
- nausea/vomiting
- haematemesis; vomiting blood
- melaena; black tarry stools
- GERD
- acid brash
- retrosternal pain
- epigastric abdominal pain
Define gastritis? What is an ulcer and how does it form?
- mucosal inflammation leading to:
- mucosal breakdown leading to
- peptic ulcer disease (duodenal and gastric ulcers)
- mucosal layer breaks down from fissure to erosion to ulcer ie exposed tissue
State the pathogenesis of ulcer disease
- acid
- diet; spicy foods/ coffee
- alcohol
- H. pylori
- NSAIDS
- Zollinger-Ellison syndrome; gastrin secreting tumour of the pancreas
What is Helicobacter pylori?
- major causative factor of PUD
- motile, flagellated ; adheres to gastric mucosa
- spiral cocbacillus
- microaerophilic; o2 is dangerous to it so must survive without it
- urease producing
Describe the importance of the urease reaction in HP?
uses chemotaxis to avoid areas of low pH
- UREASE: neutralises acid in its environment by producing large amounts of urease which breaks down urea to CO2 and NH3
- NH3 then utilises stomach acid to NH4+ ie neutralises the acid
- urease is highly immunogenic ie causes local inflammation which RESULTS IN chronic infection
How does HP damage the stomach/ duodenal linings?
- the ammonia produced to regulate pH is toxic to epithelial cells,
- so are HP proteins EG proteases, vacuolating cytotoxin A (VacA)
- they damage the epithelial cells, disrupts tight junctions and cause apoptosis
-
Cytotoxin associated gene CagA can also cause inflammation+ carcinogenic
*
How can HP be diagnosed?
- UREA BREATH TEST
- Blood test for antibodies
- Stool test; check for an antibody against any antigens of HP
- endoscopy to see if there is a peptic ulcer
Describe the varied phenotype of HP ie how does it affect different people ie manifest itself?
- gastritis only
- intermittent gastric ulcers
- intermittent duodenal ulcers
- gastric cancer
- MALT lymphoma
*
What conditions are associated with the different locations of HP?
1) Antrum only - duodenal ulcer
2) Antrum and body-asymptomatic
3) Body only- gastric ulcer leading to dysplasia in mucosa and cancer
Why do duodenal ulcers result from HP colonising the antrum only?
- Because the antrum is closer to the duodenum
- a large amount of acid goes into the duodenum from the antrum, when it should normally be neutralised at this stage
- Metaplasia occurs in the duodenal lining
What is dysplasia ( in context of gastric ulcers and cancer)?
presence of an abnormal type of tissue which can preceed cancer development stage
Why does HP colonize different areas?
- The localisation of colonisation of HP , which affects the location of the ulcer, depends on the acidity of the stomach ie depends on the individual normal production of acid
- in people producing lots of acid: HP colonises away from acidic area in the pyloric antrum to avoid acidic parietal cells near fundus
- in people producing less acid: could be because of meds eg PPI Omeprazole
- inflammatory response caused by bacteria colonizing near the antrum, induces G cells to secrete gastrin which sitmulates parietal cells in fundus to secrete acid
Why is a bacterium that only colonises gastric mucosa, implicated in duodenal ulceration?
- If HP is in the antrum, near the duodenum,
- then the G cells in the antrum will produce more gastrin; this stimulates HCl production
- Therefore there is increased HCl production from parietal cells into the antrum
- Increased HCl from the antrum passes straight into the duodenum
- causes gastric metaplasia; favourable environment for HP
- therefore allows HP to colonise duodenum ie duodenitis and ulceration
How do NSAIDS cause PUD?
- gastric mucosa protects itself from gastric acid with a layer of mucus, the secretion of which is stimulated by certain prostaglandins
- NSAIDS which are COX1 inhibitors therefore prevent production of these prostaglandins . COX1 inhibitors are worse than COX2 inhibitors
- COX-2 selective anti-inflammatories eg CELECOXIB preferentially inhibit cox-2
this is less essential in the gastric mucosa and roughly halve the risk of NSAID-related gastric ulceration
Summarise briefly the mechanism of prostaglandins
- Prostaglandins stimulate mucus and bicarbonate production
- they also cause vasodilation of nearby blood vessels, this increases blood flow
- this increases epithelial cell growth which inhibits acid secretion
How are HP and NSAIDS linked together in causing ulcers?
- HP and NSAIDS are synergistic
- ie if you have HP and you take NSAIDS, your risk of ulcers increases highly
- Ulcers and GI bleeds happen in people> 65 years on NSAIDS/ aspirin
- THEREFORE give PPIs ( to decrease acid secretions from parietal cells) for eldery NSAID patients (BUT PPIs have side effects on the liver so monitor with blood tests)
How does presentation of ulcers in different places vary?
1) Gastric Ulcers: -pain while eating
- heart burn if higher up in the antrum
- extra gastrin production; can get reflex
2)Duodenal ulcers: -pain is relieved by eating but returns after
-eg wake up in the middle of the night hungry and with pain ie need food to relieve pain
3) Pyloric Sphincter: if you have a peptic ulcer here, it can erode blood vessels
-causes a PYLORIC OBSTRUCTION because of pyloric ulcers close to the pyloric sphincter
you can vomiting and difficulty digesting your food
What are the endoscopic findings of PUD?
ulcers which are lifelong may initially asymptomatic BUT over time, they erode away and affect blood vessels
therefore cause bleeding and rarely; perforation
- you can also get SQUIRTING ULCERS:
- Ulcer erodes into artery
- blood squirts out ie heavy bleed is an emergency!
- if a slight bleed; you only get malaena
- if a TINY bleed; you get some anaemia
Name 5 main causes of upper GI bleeds?
- Peptic ulcers
- Gatroduodenal erosions
- Oesophagitis
- Mallory Weiss tear; persistent vomiting over 24 hours causes a tear in stomach from stress of vomiting ]
- Oesophageal varices
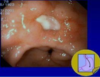
Describe the appearance of a clean gastric ulcer
- nice rolled edges
- mucosa is normal till sloughy base
- flat based pigmented spot ie low rebleeding risks
What is the appearance of a duodenal bulb ulcer?
caused by increased acid secretion

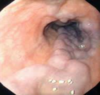
Describe the endoscopic appearance of oesophaeal varices?
- higher up
- normal mucosa on the ends
- varices are lacerated and filled with blood
*
What are symptoms and signs of an upper GI bleed? ( eg varices)
How would you treat if it was a medical emergency?
- haematemesis (can be altered)
- malaena
- increased blood loss
- normally a medical emergency because of fear of patient getting shock
- diziness eg postural hypotension/fainting
- cool and clammy, delayed CRT
- hypotension/ tachycardia ie shock
- low JVP
Treatment:
- immediate blood transfusion
- stop warfarin if patient uses it ( bc this would exacerbate bleeds)

