Session 2: Neurones and the Environment of the CNS Flashcards
Describe the network of neurones and glia
Network of neurones with supporting glia
The neurones in the brain form only a small proportion of the overall volume of the brain, and over 50% of the volume of the brain is actually formed by glial cells, acting to support, nourish, insulate, and remove the waste of neurones. There is a ratio of around 10:1 of glial cells to neurones.
Neurones sense changes and communicate with other neurones (around 10^11) neurones
Glia support, nourish and insulate neurones and remove ‘waste’ – (around 10^12) neurones
What are the types of glial cells?
Astrocytes
- Most abundant type of glial cell
- Supporters
Oligodendrocytes
- Insulators
Microglia
- Immune response
What are the roles of astrocytes
Structural support
Quick removal of neurotransmitters
Maintenance of ionic environment
Help to form blood brain barrier but do not actually form it themselves.
Describe the structural support role of Astrocytes
Structural support
Help to provide nutrition for neurones
Neurones require glucose constantly as they cannot store or produce glycogen. To overcome this, the surrounding astrocytes provide a direct source of either glucose or lactose to be transferred to the neurone. Consequently, this action allows for an additional source of energy (from the lactate) for the neurone and during any ischaemia the neurone has a store of lactose of about 5 minutes.
A direct path is seen from the endothelium to neurone by the direct path, yet the astrocyte also has a store of lactate via the glucose-lactate shuttle. This provides the additional source of lactate when required (which means any area of the brain with high energy consumption can receive adequate additional energy via this mechanism).

Describe the quick removal of neurotransmitters role of astrocytes
Remove neurotransmitters (uptake) quickly – control concentration of neurotransmitters (especially important for glutamate (toxic if present in high concentrations)).
Re-uptake: Astrocytes contain transporters specific for neurotransmitters such as glutamate, which can remove the neurotransmitter following an AP, allowing extracellular concentrations of that neurotransmitter to remain low. These neurotransmitters can then be recycled back via the astrocytes by converting them to glutamine.
The maintaining of a low concentration allows for minimal glutamine spread to other receptors of other neurons and preventing any excessively high concentration of glutamate (which can be toxic). Too much glutamate would excite the neurones too much causing Ca2+ entry which can be toxic or it can excite neighbouring neurones (undesired).
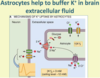
Describe the maintenance of ionic environment role of astrocytes
Maintain ionic environment - extracellular [K+] buffering. A high extracellular K+ concentration around a neuron can result in its depolarisation. Consequently, astrocytes remove K+ ions from the extracellular fluid to keep this ECF concentration low; as a result, astrocytes have a very negative resting membrane potential due to their high intracellular potassium levels. Astrocytes are coupled together by gap junctions.
What is the role of Oligodendrocytes?
Responsible for myelinating axons in CNS
They contain numerous processes that extend out and allow for the myelination of multiple neurones.
(Schwann cells are responsible for myelination in the PNS
Describe the role of microglia
Immunocompetent cells, derived from mesoderm (other glial cells are of ectodermal origin)
Recognise foreign material – become activated
Phagocytosis to remove debris and foreign material
Brain’s main defence system (due to phagocytosis)
Describe the Blood Brain Barrier
Limits diffusion of substances from the blood to the brain extracellular fluid
Maintains the correct environment for neurones
Brain capillaries have
- Tight junctions between endothelial cells. These tight junctions (bound by clodin and occludin proteins) prevent hydrophilic molecules entering through the capillaries.
- Basement membrane surrounding capillaries
- End feet of astrocyte processes. Astrocytes do not form the barrier but they send chemical messages that tell the endothelial capillaries to form tight junctions.
Due to the tight junctions that exist with the capillaries, specialised transporters need to be put in place to allow the movement of needed molecules across the BBB (this appears to be controlled by signals released from the astrocytes). Substances such as glucose, amino acids, and potassium are transported transcellularly across the BBB, allowing their concentrations to be controlled. Gaseous molecules and H2O can diffuse freely across the BBB, as will any lipophilic molecules

How is the CNS Immune Privileged?
: Immune privileged (immune specialised)
Does not undergo rapid rejection of allografts
Rigid skull will not tolerate volume expansion – too much inflammatory response (i.e. swelling) would be harmful
Microglia can act as antigen presenting cells (to T cells) as well as phagocytose foreign material
T-cells can enter the CNS
- CNS inhibits the initiation of the pro-inflammatory T-cell response - The CNS has a regulated inflammatory response, whereby T-cells are able to enter the CNS yet their inflammatory T cell response is significantly limited. Any inflammatory expansion in the CNS would not be tolerated due to the rigidity of the skull, so inflammatory responses are limited.
Immune privilege is not immune isolation, rather specialisation (to control immune response)
Describe the typical structure of a neurone
Typical neuronal structure
Cell soma
Dendrites (normally receive synaptic input)
Axon
Terminals
The axonal hillock is where the action potential is generated to pass along the axon.

Describe neurotransmitter release
Neurotransmitter release: the synapse
Action potential leads to depolarisation in the presynaptic terminal which opens voltage-gated Ca2+ channels. Influx of Ca2+ ions enter the terminal.
Vesicles fuse and release transmitter.
Neurotransmitter diffuses across the synaptic cleft and binds to receptors on the postsynaptic membrane

What does the postsynaptic response depend on?
Postsynaptic response: depends on
Nature of transmitter
Nature of receptor
Ligand-gated ion channels
G-protein-coupled receptors
A single neurotransmitter can have a number of different receptors e.g. ACh has both nicotinic and G-Protein Coupled Receptors.
What are the types of neurotransmitters in the CNS?
>30 neurotransmitters have been identified in the CNS
Can be divided into 3 chemical classes:
Amino acids: glutamate, GABA, glycine
Excitatory amino acids include glutamate (main one). It is the major excitatory neurotransmitter – over 70% of all CNS synapses are glutamatergic (most abundant) and are present throughout the CNS.
Inhibitory amino acids include GABA and glycine
Gaba is the main inhibitory transmitter in the brain
Glycine acts as an inhibitory neurotransmitter mostly in the brainstem and spinal cord
Biogenic amines: acetylcholine, noradrenaline, dopamine, serotonin (5-HT), histamine
Mostly act as neuromodulators, confined to specific pathways (not present throughout the CNS)
Peptides: dynorphin, enkephalins, substance P, somatostatin, cholecystokinin, neuropeptide Y. Dynorphin, enkephalins and substance P are all involved in pain regulation. Somatostatin, cholecystokinin and neuropeptide Y also have roles in the GI system.
Describe Glutamate Receptors
Glutamate receptors can be either Ionotropic or metabotropic
- Ionotropic have an integral ion channel – permeable to Na+ and K+ (and in some cases Ca2+ - crucial for NMDA function) ions
AMPA receptors: Na+/K+ (responsible for very fast response)
Kainate receptors: Na+/K+
NMDA receptors: Na+/K+ and Ca2+ (slower response)
Activation of ionotropic channels causes depolarisaton – increased excitability
- Metabotropic: mGluR1-7
G-protein coupled receptor
Linked to either:
Changes in IP3 and Ca2+ mobilisation
Or inhibition of adenylate cyclase and decreased cAMP levels
Describe Fast Excitatory Responses
Excitatory neurotransmitters cause depolarisation of the postsynaptic cell by acting on ligand-gated ion channels
Excitatory postsynaptic potential (EPSP)
Depolarisation causes more action potentials to be triggered.

Describe Glutamergic Synapses
Glutamatergic synapses have both AMPA and NMDA receptors (tend to exist together at the synapse)
AMPA receptors mediate the initial fast depolarisation
NMDA receptors are permeable to Ca2+
NMDA receptors need glutamate to bind and the cell to be depolarised to allow to flow through the channel – slower response but this avoids Mg2+ ions plugging the hole.
Also glycine acts as a co-agonist
Entry of Ca2+ during NMDA receptor activation can cause cell damage if intracellular Ca2+ levels become too high. Consequently, excessive amounts of glutamate can cause cell death, known as excitotoxicity.
Describe the role of Glutamate receptors in learning and memory
Glutamate receptors, synaptic plasticitiy and excitotoxicity
Glutamate receptors have an important role in learning and memory
Activation of NMDA receptors (and mGluRs) can up-regulate AMPA receptors
Strong, high-frequency stimulation causes long term potentiation (LTP) – strengthening a synapse => creates a memory (shared synaptic response)
Ca2+ entry through NMDA receptors important for induction of LTP
Too much Ca2+ entry through NMDA receptors causes excitotoxicity
- Too much glutamate – excitotoxicity
- The spread of depolarisation could activate NMDA receptors around the infarct in stroke, causing further damage.
Describe the role of glycine
Glycine is present in high concentration in the spinal cord and brainstem
Inhibitory interneurones in the spinal cord release glycine
Glycine acts on the antagonist neurone receptor, inhibiting hamstring contraction => relaxation (in the picture)

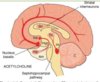
Describe Cholinergic Pathways in the CNS
Neurones originate in basal forebrain and brainstem (nucleus basalis)
Diffuse projections to many parts of cortex and hippocampus
Also local cholinergic interneurones e.g. in corpus striatum
Arousal, learning and memory, motor control
- Septum nuclei project to hippocampus – involved in learning and memory
- Basal forebrain nuclei – involved in arousal
Degeneration of cholinergic neurones in the nucleus basalis of Meynert is associated with Alzheimer’s disease
Cholinesterase inhibitors are used to alleviate symptoms of Alzheimer’s disease
Describe Dopaminergic Pathways in the CNS
Dopaminergic pathways in the CNS:
Nigrostriatal pathway is involved in motor control – important in Parkinson’s
Mesocortical and mesolimbic pathways – involved in mood, arousal and reward.
*Am: Amygdala – responsible for mood and emotions

What are conditions associated with Dopamine Dysfunction?
Parkinson’s disease
- Associated with loss of dopaminergic neurones
- Substantia nigra input to corpus striatum
- Can be treated with levodopa – converted to dopamine by DOPA decarboxylase (ADC)
- Carbidopa cannot cross the BBB whilst L-DOPA, precursor of dopamine, can cross BBB.
- Inhibiting AADC avoids too much dopamine
Schizophrenia
- Maybe due to release of too much dopamine
- Amphetamine releases dopamine and noradrenaline – produces schizophrenic like behaviour. Other neurotransmitters are probably also invovled.
- Antipsychotic durgs are antagonists at dopamine D2 receptors

Describe NA and behavioural arousal
NA and behavioural arousal
- Neurones are discrete but have many synaptic endings.
- Most NA in the brain comes from a group of neurones in the locus ceruleus
LC neurones inactive during sleep
Activity increases during behavioural arousal
Amphetamines increases release of noradrenaline and dopamine and increase wakefulness
- Relationship between mood and state of aorusal
Depression may be associated with a low state of arousal and with a deficiency of NA

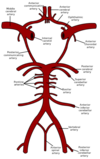
What is the Circle of Willis?
The brain is supplied by anastamoses between the internal carotid arteries (ICA) and the vertebral arteries, which anastamose at the Circulus Arteriosus / Circle of Willis. The anterior and posterior communicating arteries complete this circulation and the cerebral and cerebellar arteries given off run in the subarachnoid space. The Circle of Willis provides sufficient anastamosis so in theory any blockage of one of the arteries will allow sufficient blood supply still able to reach perfuse the region. This anastomosis may provide a collateral circulation should one of the arteries become progressively blocked, but is usually inadequate following sudden occlusion of the cerebral vessels (cerebral thrombosis, cerebral haemorrhage, cerebral embolism) and vascular stroke is a common result.
Describe the route of the ICA and vertebral arteries
The ICA runs in the carotid canal of the petrous temporal bone, passing through the cavernous sinus, to enter the middle cranial fossa. It divides into the anterior and middle cerebral arteries, with the posterior communicating artery branching off to join the posterior cerebral artery.
The vertebral arteries ascend through the transverse foramen in the upper 6 cervical vertebrae and enter the posterior cranial fossa via foramen magnum. The two vertebral arteries unite to form the basilar artery at the lower border of the pons; this then bifurcates to form the posterior cerebral arteries.

Describe the Cerebral Cortical Supply
Anterior Cerebral Arteries supply the medial surfaces of the frontal and parietal lobes, continuing to the parieto-occipital sulcus, and also supplies the leg area of the motor and somatosensory cortex
Middle Cerebral Arteries supply the lateral surface of the cerebral cortex and is the larger branch of the ICA. It supplies most of the dorsilateral surface, the motor and sensory area of the ‘central sulcus’ (except the ‘leg area’) and also supplies the speech and language areas
Posterior Cerebral Arteries supply the inferior surface of the brain and the occipital lobes and are the terminal branches of the basilar artery
Anterior cerebral artery = blue
Middle cerebral artery = pink
Posterior cerebral artery = green

Describe the Cerebellar Blood Supply
The pontine arteries come off the basilar artery and supply the pons and adjacent regions of the brain.
The arterial supply to the cerebellum comes from the superior cerebral artery (terminal branch of basilar artery), anterior inferior cerebellar artery (branch of the basilar artery), and the posterior inferior cerebellar artery (branch of the vertebral arteries).

Describe the venous drainage
The venous drainage of the brain comes via cerebral veins and the venous sinuses, all eventually draining into the internal jugular vein (IJV).
The cerebral veins can be divided into external and internal; the external (bridging) veins are in the subarachnoid space and the internal veins (draining the deeper structures) emerge from the transverse fissure. The bridging veins must cross the subdural space to drain into the venous sinuses found within the dura mater layers, which has an accompanying risk of subdural haemorrhage following any head trauma. To enter the venous sinuses the cerebral veins cross the subarachnoid space where they may be ruptured e.g. following head trauma, leading to a subarachnoid haemorrhage

Describe the dura mater. What are the venous sinuses and falx cerebri?
The dura mater is bilaminar as it contains a periosteal layer and a meningeal layer (a strong fibrous membrane), which attach adherently except where the dural venous sinuses intervene. The dura mater is a thick parchment-like membrane arranged as an outer periosteal layer and an inner meningeal layer. The periosteal layer (continuous with the cranial foramina) is attached to the bones of the skull and vertebral column and protects the brain and spinal cord by suspending them within their bony casings.
The venous (dural) sinuses are spaces between the periosteal and meningeal layers. These sinuses, including the inferior & superior sagittal, straight and transverse sinuses link the venous drainage of the brain into the internal jugular veins.
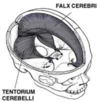
The meningeal dura mater is infolded to form a septa between the two hemispheres of the brain to form the falx cerebri; the falx cerebri attaches from the crista galli anteriorly and the horizontal tentorium cerebelli.
The tentorium cerebelli roofs the posterior cranial fossa and separates the cerebellum and the cerebral occipital lobes, providing vertical reinforcement to the cerebrum and subsequently divides the brain into supratentorial and infratentorial regions. The concave anteromedial border of the tentorium cerbelli is a free edge, producing the tentorial notch, through which the brainstem can extend from the posterior to the middle cranial fossa.
Extensions of the meningeal layer, the falx cerebri and the tentorium cerebelli, stabilise the brain laterally and vertically.
The arterial supply to the dura mater comes from mainly the middle meningeal artery. Emissary veins connect the dural venous sinuses (found between the two dural mater layers) to the veins outside the cranium.
Describe the Arachnoid Mater, Pia Mater and the Subarachnoid Space
The arachnoid mater is a delicate thin impermeable, avascular membrane, which bridges the sulci and fissures and is pressed against the inner surface of the dura by the pressure of the CSF.
The arachnoid mater consists of a thin membrane attached to the underside of the dura, and a web of tissue strands (trabeculae) which not only attaches the meningeal dura to the pia mater but creates a space (the subarachnoid space) which contains CSF.
The pia mater is the innermost fibrous layer that tightly clings to the contours of the brain and is impermeable to fluids. Together, the pia and arachnoid mater are known as the leptomeninges.
Between these two layers lies the subarachnoid space, which contains the CSF as well as cerebral arteries and veins; the space is bridged by trabeculae. Arachnoid granulations (collections of arachnoid villi) protrude through the meningeal layer of the dura mater into the dural venous sinuses and allow reabsorption of CSF into the venous circulation from the subarachnoid space.

What is a lumbar puncture? What does epidural anaesthesia involve?
A lumbar puncture is an important diagnostic tool for evaluating CNS disorders by withdrawing of CSF fluid from the lumbar cistern. The needle is inserted between L3 and L4 vertebrae (where there is no chance of damaging the spinal cord) and passes through the supraspinous ligament, ligamentum flavum, then puncturing the dura mater and arachnoid mater to enter the lumbar cistern. They should not be performed if any chance of a raised ICP.
Epidural anaesthesia involves administering the anaesthetic agent into the epidural space, so it can bathe the nerve roots. Spinal anaesthesia can also sometimes be given.

Describe the movement of CSF
Cerebrospinal Fluid (CSF) is secreted by choroid plexus cells, which line all the ventricles (mainly in the lateral ventricles), via an energy-dependant process (not simply a filtrate of blood), and lies in the subarachnoid space and ventricular system.
The movement of CSF is from:
- Lateral ventricles to the third ventricle via the Foramina of Monro
- Third ventricle to the fourth ventricle via the cerebral aqueduct
- Fourth ventricle to the subarachnoid space via foramen of Luschka / median aperture or cistern magna via foramen of Magendie / lateral aperture
The CSF can then travel rostrally over the cerebral hemispheres where it enters the arachnoid villi. The arachnoid villi allow flow of CSF into the dural venous sinuses, but not in the opposite direction as the pressure in the subarachnoid space is higher than that in the dural sinuses.

Describe the Ventricular System
The brain’s ventricular system is composed of 4 cavities (known as ventricles), including two lateral ventricles, a third ventricle, and a fourth ventricle. Each lateral ventricle corresponds to the shape of a cerebral hemisphere, which is composed of anterior horn, body, posterior horn, and an inferior horn. The third ventricle occupies the midline and the fourth ventricle is located posterior to the pons and upper half of the medulla, ventral to the cerebellum.
