Porth: Chpt. 28 Flashcards
What is the GI Tract also referred to as?
- Digestive Tract
- Alimentary Canal
- Gut
What is the Intestinal Portion of the GI Tract called?
- Bowel
Name the Accessory Organs that produce secretions & aid in digestion?
- Pancreas
- Liver
- Salivary Glands
Major Physiologic Functions of the GI Tract
- Digest food
- Absorb nutrients
How does the GI Tract carry on the functions of digestion & absorption?
- Motility
- Secretion
- Digestion
- Absorption
What happens to the Unabsorbed Nutrients & Wastes in the Large Intestine?
- Collected
- For later elimination

What must Nutrients do in order to become part of the body’s Internal Environment?
- Pass through Intestinal Wall
- Enter Blood & Lymph Channels
For Simplicity’s Sake:
What are the 3 parts of the GI Tract?
- Upper part
- Mouth, Esophagus, Stomach
- Intake source & Receptable
- 1st portion of digestive process
- Mouth, Esophagus, Stomach
- Middle part
- Duodenum, Jejunum, Ileum
- Digestion & Absorption!
- Duodenum, Jejunum, Ileum
- Lower part
- Cecum, colon, recturm
- Storage channel
- Elimination of waste
- Cecum, colon, recturm
Which President signed Father’s Day into Law?
- 1966, President Lyndon B. Johnson issued the first presidential proclamation honoring fathers, designating the third Sunday in June as Father’s Day.
- Six years later, the day was made a permanent national holiday when President Richard Nixon signed it into law in 1972.
What does Saliva do?
- Moisten & lubricates food
- Eaiser to Swallow
- Enzymes
- Initial digestion of Lipids and Starches
The Esophagus
- 25cm, straight, collapsible tube
- Connects oropharynx w/ stomach
- Conduit for passage of food
- Smooth muscle = Peristalsis!
- Mucosal/Sub-mucosal glands = Protects surface, lubricates food
The Esophagus
&
Its Sphincters
- 2: Upper & Lower
-
Upper = pharyngoesophageal
- Striated muscle
- Keeps air from entering stomach
-
Lower = gastroesophageal
- Circular muscle
- Tonically contracted
- Zone of high pressure
- Prevents reflux
- Passes through hiatus in diaphragm to join w/ stomach
-
Upper = pharyngoesophageal
The Esophagus
&
“Receptive Relaxation”
-
Lower = gastroesophageal sphincter
- Allows propulsion of esophagus contents into stomach
- Hiatus region = high pressure
- Prevents reflux

The Stomach
-
Pouchlike structure
- Food storage reservoir

The Stomach
+
Cardiac Orifice
Where esophagus opens into stomach

The Stomach
+
Pyloric Sphincter
End of pyloric canal
Circular, Smooth muscle
Valve = controls rate of stomach emptying
+ Prevents regurgitation of intestinal contents into stomach
Middle GI Tract
-
Duodenum:
- 22cm long
- Connects Stomach to Jejenum
- Opening for Common Bile Duct + Main duct
- Juices enter via ducts
-
Jejunum & Ileum:
- 7m (23ft) long [folded]
- DIGESTION & ABSORPTION!
Lower GI Tract
- Large intestine = 1.5m (5ft) long
- Cecum, Colon, Rectum, Anal Canal
- Cecum = Pouch @ junction btwn Ileum & Colon
- Valves - prevent return of feces into small intestine
- Appendix = 1in from ileocecal valve
- Colon
- Descending colon extends to rectum
- Rectum = sigmoid colon to anus
- Anal Canal = btwn levator ani muscles
- Spinchter muscles = no incontinence
How fast does a crack in glass travel?
When glass breaks, the cracks move faster than 3,000 miles per hour!!!
GI Wall Structure
The Digestive Tract is a __________ tube

-
Four-Layered Tube
- Inner Mucosal Layer
- Epithelium, Lamina propria, Muscularis mucosa
- Submuscosal (2nd layer)
- Connective & Adipose
- Muscularis externa (3rd layer)
- Serosal (4th layer)
- Mesothelium (squamous)
- Inner Mucosal Layer
GI Wall Structure
Inner Mucosal Layer - Functions
- Lubricates & Protects inner surface of alimentary canal
- Secretes digestive enzymes
- Break down food
- Absorb breakdown products
- Prevents entry of bad substances
- Lymphatics in here = 1st line of defense
GI Wall Structure
Inner Mucosal Layer - Epithelial Lining
- Rapid turnover rate
- Replaced q 4-5 days
- Heals rapidly
- No scar tissue
GI Wall Structure
Second Layer - Function
- Secretes digestive enzymes
- Has lots of vasculature
GI Wall Structure
Third Layer - Function
- Circular smooth muscle cells
- AND
- Longitudinal smooth muscle cells
- =’s
- Facilitate MOVEMENT of GI Tract contents
- =’s
GI Wall Structure
Fourth Layer - Function
- Equivalent to:
- Visceral Peritoneum
- Most superficial layer of digestive tract parts suspended in peritoneal cavity

The Peritoneum
Largest serous membrane in the Body!
2 layers;
- Visceral
- Parietal
The Peritoneum
What is between the 2 layers of the Peritoneum?
Peritoneal Cavity!
“Potential Space containing serous membrane fluid”
Moint & Slippery Surface - preventing Friction!
The Mesentery
Double layer of peritoneum
Encloses abdominal viscera & attaches it to the abdominal wall
-
Contains: Blood vessels, nerves, lymph vessels
- Supply intestinal wall
- Holds organs in place
- Stores Fat

The Omentum
- Double-layered extension of peritoneum
- Passes from stomach or proximal part of duodenum to adjacent organs in abdominal cavity/wall
- Greater Omentum
- Lesser Omentum

The Omentum
Greater Omentum Functions
- Contains fat
- can be A LOT in obese people
- Mobile
- Moves around in cavity w/ peristatsis of intestine
- Forms adhesions
- Fiborous scar tissue
- Walls of infection & prevents spread
- Cushions & Insulates!

Which Continent contains the most Deserts?
- Antarctica
- Antarctica is considered a desert, with annual precipitation of only 200 mm (8 inches) along the coast and far less inland

The movements of the GI Tract can be:
Rhythmic & Tonic
-
Rhythmic
- Intermittent contractions
- Mix & Moves food along tract
- esophagus, antrum, small intestine
-
Tonic
- Constant level of contraction w/o relaxation
- lower esophagus, upper stomach region, ileocecal valve, internal anal sphincter
What parts of the GI Tract are NOT made of Smooth Muscle?
- Pharynx
- Upper 1/3 of Esophagus
- External Anal Sphincter
Basic Properties of the GI Tract Smooth Muscle
- Cells electronically coupled by low-resistance pathways
- =’s electrical signals that contract muscle move quickly from one fiber to the next!
- Pacemaker cells
- Rhythmic, spontaneous oscillations
- SLOW WAVES
- Enteric Nervous System run this
- Located in GI Tract wall
- PNS and CNS
- Peptides, NTs, Hormones assist in Motility!
- Rhythmic, spontaneous oscillations
Enteric Nervous System
- Myenteric & Submucosal Plexuses in wall
- Nerve fibers & ganglion cell bodies
Enteric Nervous System
Myenteric Plexus
- Linear chain of interconnecting neurons
- Btwn longitudinal & circular msucle layers
- Runs all way down wall
- Motility along length of gut!

Enteric Nervous System
Submucosal Plexus
- Btwn mucosal & muscle layers of intestine
-
Controls function of each segment of intestinal tract
-
Local control of
- Motility
- Intestinal Secretions
- Nutrient Absorption
-
Local control of

Enteric Nervous System
Myenteric & Submucosal Plexuses
Regulation
- Local influences
- Input from ANS
- Interconnecting Fibers transmit Info
- Mechanoreceptors
- Monitor stretch & distention
- Chemoreceptors
- Monitor chemical composition (pH, osmolality…)
Which Insect has the Longest Life Span?
A queen termite has been known to live 50 years….gross!

What mediates the Autonomic NS of the GI System?
Sympathetic & Parasympathetic NS
- Parasympathetic NS = Increase in Enteric NS activity
- Sympathetic NS = Inhibits Activity
Parasypathetic Inneveration occurs through what nerve?
Vagus Nerve
(+ some of the colon is innvervated by fiber that exits via sacral region of spinal cord)
Preganglionic Parasympathetic Fibers
Synapse w/ Plexus Neurons
(or) Act directly on Intestinal Smooth Muscle
+ Provide afferent nerves!
Receptors lie w/in various gut tissue
These nerves project to spinal cord & brain
=’s Sensory Input for Integration
Most Parasympathetic Innervation is….
Excitatory!
How does Sympathetic Innveration occur?
Via Thoracic chain of sympathetic ganglia, superior mesenteric, inferior mesenteric ganglia.
Sympathetic Innveration
- Controls extent of mucous secretion by mucosal glands
- Reduces motility
- (inhibits activity of intramural plexus neurons)
- Enhances sphincter function
- Increases vascular smooth muscle tone of blood vessels
Sympathetic Innveration
&
Its effect
Blocks release of the excitatory neuromediators in intramural plexuses, which inhibits GI Motility!

What begins the Digestive Process?
Chewing!
Breaks food into small particles to swallow
Lubricates it w/ salvia
Mixes starch food w/ Salivary Amylase

Swallowing…
Voluntary, or Involuntary?
- Initiated as Voluntary
- Becomes involuntary when reach Pharynx

Where is the “Swallowing Center”?
- Reticular formation of the medulla and lower pons
- Responds to the Tactile receptors in pharynx & esophagus
- Turns into motor response via Medulla & Pons
- Responds to the Tactile receptors in pharynx & esophagus
What nerves carry out the Swallowing Phases?
- V, IX, X, XII
- oral & pharyngeal
- X
- esophageal
If you damage the nerves that help you swallow - What are you at risk for?
- Asphyxiation
- Aspiration pneumonia
Three Phases of Swallowing
- Oral
- Voluntary
- Bolus touches pharynx
- Pharyngeal
- Epiglottis covers larynx
- Bolus moved by constrictive pharynx movements
- Involuntary!
- Esophageal
- Peristalsis triggered as Esophagus walls are stretched
2 Types of Peristalsis
- Primary
- Controlled by swallowing center
- When food enters esophagus
- Secondary
- Mediated by smooth muscle fibers
- Occurs when primary is inadequate
Where does Peristalsis begin and go?
- Begins: Site of distention
- Goes: Downward
- Before wave reaches stomach
- Lower esophageal sphincter relaxes & allows bolus to enter stomach
- Before wave reaches stomach
Why is it good to have greater pressure in the lower esophageal sphinter versus the stomach?
To PREVENT REFLUX of gastric contents

What’s the difference between a dirty old bus station and a lobster with boobs?
One’s a crusty bus station, and the other is a busty crustacean.

What is the creamy mixture of food in the stomach called?
Chyme

What is the Volume of an Empty Stomach?
& How big can it expand to?
- 50mL = empty
- 1000 mL (before intraluminal pressure rises)
Motility of the Stomach results in….
- Churing & mixing of solid foods
- Regulates emptying of chyme into duodenum
- Begins in Pacemaker area in middle of stomach
- Moves to Antrum (contractions increase)
- Pyloric sphincter is contracted during antral contraction
- Gastric contents emptied into dueodenum btwn contractions
Pyloric Sphincter constriction prevents
- Backflow of gastric contents
- Allowing them to flow into duodenum at a good speed/rate
Why is the prevention of backflow into the stomach important?
- Backflow of bile salts & duodenal contents =
- Damage of mucosal surface of antrum
- ULCERS!!
- Damage of mucosal surface of antrum
Neural & Humoral Signals
- Regulates stomach emptying
- Signals from stomach & duodenum
- DUODENUM = gives the strongest signals
- signals at rate to digest & absorb chyme
What slows Gastric Emptying?
- Hypertonic Solutions in the Duodenum
- Duodenal pH below 3.5
- Presence of Amino Acids, Peptides & Fatty Acids in Duodenum
Stimulation of Gastric Emptying
- Enteric NS & PNS, SNS connections mediate reflexes
- Hormones:
- Cholecystokinin & Glucose-dependent insulinotropic peptide
- slow emptying
- Cholecystokinin & Glucose-dependent insulinotropic peptide
Stimulated by: Fats (& other foods)
If Gastric motility is TOO SLOW due to Obstruction or Gastric Atony what can occur?
- Gastric Retention
Obstruction can be due to:
- Formation of Scar Tissue in pyloric area after a Peptic ulcer
- Hypertrophic Pyloric Stenosis
- in infants w/ thick muscularis layer in terminal pylorus
-
Treatment:
- Myotomy - Surgical incision of muscular ring

Gastric Atony
- Can occur as complication of Visceral Neuropathies in DM
- Distruption of Vagal Activities
Abnormally Fast Emptying
-
“Dumping Syndrome”
- Surgical complications
- characterized by:
- Rapid dumping of highly acidic & hyperosmotic gastric secretions into Duodenum & Jejunum

What is the National Animal of Scotland?
UNICORN!!!!

What Reflexes control Defecation?
- Defecation Reflexes!!
-
1. Intrinsic Myenteric Reflex
- Mediated by enteric NS
- Intiated by rectal wall distention
- Mediated by enteric NS
-
2. Parasympathetic Reflex
- Sacral Cord
-
1. Intrinsic Myenteric Reflex
- Impulses increase peristaltic movements & relax the Internal Sphincter

Which Dr. Suess Book has exactly 50 words in it?
Green Eggs and Ham!

GI Hormones
What do they influence?
- Appetite
- GI Motility
- Enzyme activity
- Electrolyte levels
- Secretion & Action of other hormones

GI Hormones
Stomach Hormones
- Gastrin
- Ghrelin

GI Hormones
Intestine Hormones
- Secretin
- Cholecystokinin
- Incretin

What does CHARGOGGAGOGGMANCHAUGGAGOGGCHAUBUNAGUNGAMAUGG mean?
It means “you fish on your side, I fish on my side, and no one fishes in the middle.”
There’s a Native American lake named Chargoggagoggmanchauggagoggchaubunagungamaugg.
This lake is located in Webster, Massachusetts.

Gastric Secretions
- Stomach has mucus secreting cells & others:
- Pariteal (oxyntic) cells
- Secrete HCl & Intrinsic factor
- Chief cells
- Secrete pepsinogen
- Initiates protein-breakdown
- Secrete pepsinogen
- G cells
- Secrete Gastrin
- Pariteal (oxyntic) cells

The average person spends 2 weeks of their lifetime waiting for the light to change from red to green.
Isn’t that refreshing?

Gastric Acid Secretion
3 Substances that Stimulate HCl secretion
- ACH (from vagal nerves)
- Gastrin (G cells)
- Histamine (endocrine cells)
Each bind to a different Parietal cell & different MOA, BUT:
-stimulate increase of H+ via Proton Pump

How long do Taste Buds last for?
Taste buds go through a life cycle where they grow from basal cells into taste cells and then die and are sloughed away.
Taste Bud’s normal life cycle is anywhere from 10 days to two weeks.

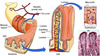
Digestion
Villi of the Small Intestine
&
Where do digested Molecules go?
- Diffuse through membrane
- or
- Actively transported across mucosal surface to enter blood (fatty acids enter luteal)
- Molecules are transported through portal vein or lymphatics into systemic circulation
What Animal is the Sleepiest in the World?
The koala sleeps 22 hours a day!
Next is the sloth (20 hours), armadillo and opossum (tied at 19 hours each), lemur (16 hours), then hamster and squirrel (tied at 14 hours each).

Carbohydrate Digestion & Absorption
Carbohydrate Breakdown chart

Fat Digestion & Absorption
What do you call Fat that is NOT absorbed into the Intestine?
-
Steatorrhea
- Excreted in the stool
- >20g+ of fat in stool in a 24-hour stool sample

The Chapter is almost DONE!!
Wahoo!
