Miscellaneous: FMD, other aneurysms, AV malformation, peds, tumours Flashcards
What vessels does fibromuscular dysplasia affect?
Most medium sized arteries - e.g. internal carotid and renals
What layer of the vessel does fibromuscular dysphasia affect?
Media
What is the prevalence of fibromuscular dysphasia?
Unknown
Who gets fibromuscular dysphasia? (Age, sex)
Young females
What is the theory for pathogenesis of fibromuscular dysplasia?
Ischemia of vasovasorum. Arteries affected are internal carotid, vertebral and renals that have long segments without branch points thus less vasovasora.
What is the definition of nutcracker syndrome?
Compression of left renal vein by SMA. Nutcracker syndrome = constellation of symptoms. NC phenomenon if asymptomatic.
What are risk factors of nutcracker syndrome?
Low BMI, young female
How can low BMI lead to nutcracker syndrome?
Paraspinal muscle wasting and low mesenteric/retroperitoneal fat means that SMA is at a more acute angle <16 degrees vs normal 35-40 degrees
What are the 3 anatomical types of nutcracker syndrome?
Anterior and posterior. Also “atypical” circumaortic renal vein or congenital malformations e.g. left IVC
What is posterior nutcracker syndrome
Usually with retroaortic vein, compression of left renal vein against vertebral body
What are symptoms of nutcracker syndrome?
Hematuria and left flank pain. Also genital varices, pain with menses/sex/urination, protienuria and abdo pain
What is the duplex criteria for nutcracker syndrome?
Flow velocities/diameter proximal and distal to stenosis ratio > 5
What is the most common open operation for nutcracker syndrome?
Renal vein transposition onto the IVC more caudally. Gonadal and adrenal veins often have to be ligated.

What are open options for anterior nutcracker syndrome?
Left renal vein transposition +/- patch or saphenous vein cuff. Gonadal vein transposition. Saphenous vein bypass from LRV to IVC.
What open operations can be used for both anterior and posterior nutcracker syndrome?
Gonadal vein transposition, saphenous vein bypass from LRV to IVC
What is the rate of migration for renal vein stenting?
7%. Can possibly migrate to right atrium and require open heart surgery!
What are the differences between hemangiomas and congenital malformations?
Hemangioma = tumour, grows rapidly, involutes by age 12, originates from proliferative endothelium
Congenital vascular malformations - inborn error, grow steadily in parallel with childs growth, never disappear or regress, quiescent endothelium
What are the 6 types of congenital malformations according to the Hamburg classification?
1-Arterial
2- Venous
3-Arteriovenous shunting
4-Lymphatic
5-Combined hemolymphatic
6-Capillary
What are the congenital vascular malformation embryologic subtypes?
- Extratruncular:
- infiltrating/diffus,
- limited/localized
- Truncular:
- stenosis or obstruction (hypoplasia, aplasia, hyperplastia, membrane congenital spur),
- dilation (localized = aneurysm, diffuse = ectasia)
What abnormality is depicted here?

Portwine stain - Klippel Trenaunay syndrome. Limb swelling and leg length discrepancy. Hemolymphatic malformation.
Who gets congenital vascular malformations more? Men or women?
1:1, M:F
What is the most common type of congenital vascular malformation?
Venous
What are 5 types of risk factors during pregnancy that are associated with congenital vascular malformations?
1) Exposure to chemicals
2) Infections: rubella, herpes, toxoplasmosis
3) Drugs: thalidomide, anticonvulsants, quinine
4) Rec Drugs: EtOH, Cocaine, smoking
5) Diseases: DM, thyroid disease, TB, hypoxia, lead/carbon monoxide
When do extratruncular congenital malformations arrest development?
Early embryonic life while vascular system is in the reticular stage.
What stmulates extratruncular CVMs to grow and proliferate?y,
Internal stimulation: menarche, pregnancy hormonal release
External: trauma, surgery
Why do extratruncular CVMs behave like an infiltrating process/invade surrounding structures?
Arrested growth in early embryonic life. Bones, muscle, soft tissue and blood vessels all originate from same mesoderm and no plane of partition between them.
What has a higher rate of recurrence - extratruncular or truncular CVM?
Extratruncular
What type of CVMs are associated with more serious hemodynamic consequences? Truncular or extratruncular?
Truncular
When do truncular CVMs arise?
Arrested development later, during vascular trunk formation stage when truncular lesions have lost the characteristics of mesenchymal cells. All appear as formed vessels with various degrees of development.
What are the differences between a vascular birthmark and capillary malformations?
1- Colour: CM = port wine, birthmark = pinkish
2- Location: CM = anywhere on body, birthmark = nuchal “stork bite” or face “angel’s kiss”
3- CM accompanied by other abnormal findings beneath the skin (e.g. CM of face = warning sign of intracranial CVM Sturge Weber Syndrome with ipsilateral ocular and leptomeningeal vascular malformation)
What is Sturge Weber syndrome?
Neurologic syndrome that presents as port wine stain of face. Ipsilateral ocular and leptomeningeal vascular malformation may result in seizures, increased pressure in the eye (glaucoma), developmental delays, and weakness on one side of the body
What type of CVM is this? Soft bluish swelling. Easily compressible. Enlarge with dependency/valsalva. Respond to compression therapy.
Venous
What type of CVM is this? Ischemic changes, distal gangrene, high output heart failure
Arteriovenous
What is the marginal vein?
An embryonic tissue remnant that fails to involute - usually on lower leg and looks like a large dilated lateral vein. Often heralds coexisting deep venous anomalies which should be investigated.
What is the name of the prominent vein on the back of this patients leg?

Marginal vein (embryonic remnant failed to involute). Parker weber syndrome.
What is transarterial lung perfusion scintigraphy (TLPS)?
A scan with radioisoptope tagged albumin microspheres to measure the percentage of blood shunted by AVMs. Can be used to detect microshunting common in Park weber syndrome
Which type of congenital vascular malformations need to be treated aggressively?
Extratruncular. They grow and will recur unless the lesion nidus is completely destroyed
Which type of congenital vascular malformations can be handled conservatively unless they become hemodynamically significant?
Truncular lesions. They lack the potential for proliferation.
What are 10 indications to treat extratruncular vascular malformations?
1-Hemorrhage
2-High output heart failure
3-Cosmetically deforming
4-Vascular bone syndrome
5-Near vital structures: airway, sight/eat/hear regions
6-Recurrent sepsis
7-Disabling pain
8-Lymph leak
9-High risk regions: hemartrhrosis, DVT, PE
10-Secondary ischemic complications
What is congenital vascular bone syndrome?
Long bone abnormal growth caused by congenital vascular malformation
What do congenital vascular malformations contribute to leg length descrepency to make the affected limb longer?
AV shunts cause arterial hypertrophy and hypervascularization of the bone
What do congenital vascular malformations contribute to leg length descrepency to make the affected limb shorter?
Bone compression from vascular mass or reduction of arterial inflow from arterial hypoplasia will cause bone shortening.
How does the marginal vein relate to congenital vascular bone syndrome?
It causes angio-osteo hypertrophy and limb overgrowth
What are 4 clinical features of Klippel Trenaunay Syndrome?
1-port wine stain localized to a small area
2-limb overgrowth/gigantism
3-large cluster of varicose veins
4-large lateral venous collector (Marginal Vein)
What type of congenital vascular malformations do Klippel Trenanay patients get? Arteriovenous, venous or lymphatic?
All KTS patients get venous, lymphatic and combined hemolymphatic
How do you treat the majority of Klippel Trenaunay Syndrome patients?
Compression stockings (35-45) and sclerotherapy
What is the difference between park weber syndrome and klippel trenaunay syndrome?
Very similar. PWS associated with arteriovenous malformations that require embolization in symptomatic patients.
What is “Localized Intravascular Coagulopathy”?
Extratruncular venous malformations associated with coagulopathy due to stasis of blood within abnormal structures
What are phleboliths?
Microthrombi from localized intravascular coagulopathy associated with venous malformation that take on a “stone like” structures that you can see on plain x-rays. May be an indication to anticoagulate.
Why do congenital malformation patients need to be followed life long?
Menarche, pregnancy, hormonal therapy, trauma, or surgery can trigger activity in previously quiet lesions and they can grow rapidly
What are “high flow” congenital vascular malformations?
arteriovenous fistulas
What are “low flow” congenital vascular malformations?
Venous, lymphatic, capillary
How do you treat capillary malformations for cosmesis?
Flashlamp pulse dye laser therapy
How are macrocystic lymphatic malformations treated differently from microcystic?
Name 3 signs and symptoms of large vessel vasculitis
- Bruit
- Asymmetrc BP
- Claudication
Name 5 signs and symptoms of medium vessel vasculitis
- Cutaneous nodules
- Livedo reticularis
- Digital gangrene
- Mononeuritis multiplex
- Renovascular HTN
Name 4 signs or symptoms of small vessel vasculitis
- Palpable purpura
- Pulmonary renal syndromes (glomerulonephritis, alveolar hemorrhage)
- urticarial skin rashes
- scleritis.
Name 2 large vessel vasculitis
“Giant Samurai”
- Giant cell arteritis
- Takayasu
Name 3 medium vessel vasculitis
“Obliterating your cow in a medium sized pan”
- Thromboangitis obliterans
- Kawasaki
- Polyarteritis Nodosa
Name 5 small vessel vasculitis
Small German men who Cryo
- Henoch Schonlen Purpura (IgA vasculitis)
- Wegners (Granulomatosis w Polyangitis)
- Cryoglobunimeic vascultis
- Churg Strauss (Eosinophilic granulomatosis w polyangitis)
- Microscopic polyangitis
Is giant cell arteritis more common in men or women?
Women (life time risk 1% for women, 0.5% for men)
What are the diagnostic criteria for giant cell arteritis?
3 of 5:
- Elevated ESR
- Age > 50
- Temporal abnormality (e.g. tenderness or decreased pulsation)
- New headache
- Abnormal biopsy (predominance of mononuclear cell infiltration or granulomatous inflammation with multinucleated giant cells)
What is the treatment for giant cell arteritis?
Give Cortocosteroids Always! (GCA)
IV methylprednisolone 1000 mg/day x 3 days if visual loss.
Otherwise 40-60 mg po daily.
What are classic CT findings of Ormond Disease (Idiopathic retroperitoneal fibrosis)?
Homogenous mass around the aorta following the iliac bifurcation with associated medial deviation of the mid part of the ureter and secondary hydronephrosis.
What are typical symptoms of Ormond Disease (idiopathic retroperitoneal fibrosis)?
Pain in lower back, abdomen, flank and scrotum
HTN
Systemic symptoms (fever, anorexia, malaise)
Which vasculitis is associated with a “hairy kidney”?
Erdheim Chester Disease
What feature distinguishes Erdheim Chester Disease from Ormond and IgG4 related systemic disease?
Bony lesions often of the lower extremeties that present with juxta-articular pain
What are the diagnostic criteria for polyarteritis nodosa?
3 of 10: ABCDEFGHI
- Arteriographic abnormality (aneurysms or occlusions, string of pearls)
- Biopsy of small or medium arteries showing polymorphic neutrophils.
- Cr or BUN elevated
- dBP > 90
5/6. Extremity pain (myalgia) incl. testicular pain
- Florid Livedo reticularis
- Gross weight loss > 4kg
- Hep B infection
- Impaired sensation (Mono or poly neuropathy)
Name 5 conditions that mimic polyarteritis nodosa
- Segmental arterial mediolysis (SAM)
- Pseudoxanthoma elasticum
- Neurofibromatosis
- Vascular type Ehlers Danlos (defect in Type 3 Collagen)
- Adenosine deaminase 2
What are arteriographic findings consistent with Thromboangiitis obliterans?
“Corkscrew collaterals” around areas of occlusion with normal proximal arteries without evidence of atherosclerosis or emboli
What are 2 histologic features of thromboangiitis obliterans that distinguishes it from other vasculitis?
- IEL is preserved
- Venulitis also often seen
What are treatments for thromboangiitis obliterans?
- Total cessation of all nicotine
- Calcium channel blockers
- IV iloprost
- Sympathectomy
What percentage of patients with thromboangiitis obliterans that continue to smoke require an amputation?
50%
Which vasculitis involves small vessels, associated with pANCA and associated with pulmonary renal syndrome?
Microscopic polyangitis
What is the diagnostic criteria for Eosinophilic Granulomatosis with Polyangiitis (Churg Strauss)
APE MEN (4 of these 6)
- A - asthma
- Paranasal sinusitis
- Eosinophilia
- Migratory pulmonary infiltrates on CXR
- Extravascular accumulation (e.g. nasal polyps)
- Neuropathy
What are clinical features of Bechets Disease (focus on vascular symptoms)?
BOOGIE PANTS
- Budd chiari
- Oral ulcers
- Ocular ulcers
- Genital ulcers
- Intracranial aneurysms
- Extremity aneurysms (popliteal/femoral/brachial/iliac)
- Pulmonary aneurysms - can have fatal hemoptysis
- Aortic aneurysm
- Neurologic symptoms
- Thrombosis of veins (mesenteric, hepatic, renal)
- Stomach/GI inflammation
What percentage of rheumatoid arthritis patients develop vasculitis?What percentage of rheumatoid arthritis patients develop vasculitis?
10-15%
Which vasculitis is a rare autoimmune disease manifested with recurrent inflammation of cartilaginous tissues? What vessels are involved?
Relapsing polychondritis, large-vessel (thoracic and AAA)
What is this image depicting? Which diagnosis is this a hallmark feature?

Corkscrew collateral (“dot sign”) - Buerger’s disease
Which condition is this CTA depicting?

Takayasu’s arteritis - skip lesion with inflammation of aortic wall (low attenuation ring)
What are the 9 minor diagnostic criteria for Vascular EHDS?
CHEAT FANG:
- Club foot
- Hypermobility of small joints
- Early onset varicose veins
- AV carotid-cavernous fistula
- Tendon/muscle rupture
- Family history (suddent death in one or more close relatives)
- Acrogeria (taut thin skin)
- pNeumothorax
- Gingival recessession

What are the 4 major diagnostic criteria for Vascular EHDS?
FABS:
- Facial characteristic appearance (thin delicate nose, thin lips, hollow cheeks)
- Arterial/uterine/GI rupture
- Bruising
- Skin thin/translucency

What 3 features are associated with Loeys Dietz, “classic triad”?
- Aortic aneurysm/vascular tortuosity
- Craniofacial abnormality - bifid uvula or cleft palate
- Hypertelorism

How are aortorenal bypasses approached (type of incision)?
Transverse subcostal - kidney can be exposed retroperitoneally or transperitoneally depending on extent of aorta needed to be exposed.

What are the 6 types of popliteal entrapment syndrome?
- Popliteal completes development before migration of medial head of gastroc. Gastroc is situated normally but pushes popliteal artery medially.
- Popliteal artery is displaced medially because the medial head of gastroc has an abnormal insertion site on the femoral condyle.
- Abnormal muscle slip or fibrous band from either medial or lateral femoral condyle
- Persistence of axial artery as the mature distal popliteal artery - remains in its embryologic position deep to the popliteus.
- Both popliteal artery and vein are entrapped by any of the type 1-4
- Anatomic variant not known, possible gastroc hypertrophy

Name 7 non-atherosclerotic causes of peripheral artery disease
- Popliteal entrapment
- Adventitial cystic
- Iliac artery endofibrosis
- Fibromuscular dysplasia
- Buerger’s disease
- Vasculitis (Takayasu, Giant Cell Arteritis, Behcets)
- Chronic exertional compartment syndrome

Which types of popliteal entrapment are best approached from a medial vs. posterior approach?
Medial - I and II
Posterior - III and IV

Name 5 ways of dealing with an infected femoral pseudoaneurysm
- Ligate & wide debridement (illicit drug use can ligate the femoral if SFA/profunda intact, test occlusion and see if you maintain a pedal doppler signal first)
- In-situ reconstruction with vein or cryopreserved allograft and sartorius muscle flap
- Obturator bypass
- Latera femoral bypass from external to distal SFA
- Axillary to distal SFA bypass.

Name 6 causes for pediatric aneurysms
- Infection
- Aortitis - takayasu
- Arteritis - Behcet, SLE, kawasaki, PAN
- Genetic - EDIV, LDS, Tuberous sclerosis, Marfans
- Developmental/idiopathic
- Traumatic

Name the Neves and Zincke classification of this tumour thrombus
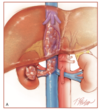
Level 3 - retrohepatic but still below the diaphragm without extension into the right atrium
Name the Neves and Zincke classification of this tumour thrombus

Level 2 - cephalad extent is more than 2 cm above the left renal vein but still infrahepatic
Name the Neves and Zincke classification of this tumour thrombus

Level 1 - cephalad extent is confined to less than 2 cm above the left renal vein
During an “en bloc ” resection of a colon cancer fecal contamination occurs and the IVC is resected 5 cm longitudinally and 50% circumferentially. List 5 ways to repair the IVC:
- Lateral venorapphy with 3-0 or 4-0 Prolene if less than 50% stenosis
- Patch repair (saphenous; prosthetic if no contamination). Patch repair preferred over interposition graft
- Interposition graft (deep femoral vein or spiral saphenous vein graft; 16 mm PTFE if no fecal contamination)
- Ligation of infrarenal IVC (unstable patient with severe injuries or when repair produces major stenosis or cancer patients with chronically obstructed IVC and developed collaterals)
- Reconstruction of IVC with cuff of abdominal aorta and subsequent aortic reconstruction with ax-fem graft or rifampin coated graft (if no fecal contamination then regular Dacron tube graft repair)

When do you need to use veno-venous bypass for IVC reconstructions? (5)
- Pt unable to tolerate IVC clamping due to tenuous cardiopulmonary status or old age
- Level 3 extension of tumour thrombous
- Complex multilevel IVC involvement
- Need full graft replacement
- Adequate oncologic resection cannnot be achieved without bypass support
When ligating vessels for a hepatic artery aneurysm, when do you also need to perform a cholecystectomy?
If the proper or right hepatic artery is ligated, a cholecystectomy should also be performed

Name 5 major theories about the pathogenesis of chronic regional pain syndrome
- Exaggerated inflammatory response - inflammatory mediators TNF-a and IL-6 are elevated in affected limbs. Red/hot/swollen affected limb are all signs of inflammation. Some benefit of IVIG.
- Sympathetically mediated syndrome
- Limb ischemia and reperfusion injury
- Central sensitization theory
- Secondary to nerve damage
- Autoimmune disorder
- Cortical reorganization theory

Name the Stanton Hicks diagnostic criteria for complex regional pain syndrome
- Clinical symptoms:
- burning, hyperpathia, allodynia
- Temperature or color changes edema
- Hair or nail growth changes
- Laboratory results
- Thermometry or thermography bone radiography
- 3 phase bone scan quantitative sweat test response to sympathetic block
Interpretation: > 6 reflex sympathetic dystrophy probable, 3-5 RSD possible, <3 RSD unlikely

Name the Budapest clinical diagnostic criteria for complex regional pain syndrome
1. Ongoing pain out of proportion to inciting event
2. 1 symptom in 3/4 categories:
i) vasomotor: tempreature asymmetry/skin colour
ii) sensory: hyperesthesia, allodynia
iii) Motor/trophic
iv) Sudomotor/edema
3. One sign in 2+ categories:
i) vasomotor: temp asymmery
ii) sensory: hyperalgesia to pin prick and/or allodynia to light touch
iii) motor/trophic: decreased ROM or motor dysfunction or trophic changes
iv) Sudomotor/edema
4. No other diagnosis better explains signs/symptoms

A 3 phase bone scan with accelerated blood flow in the disease limb combined with increased diffuse activity during the blood-pool phase and increased periartericular uptake in the delayed statis phase is pathognomonic for which condition?

Chronic regional pain syndrome. However a meta-analysis states bone scans have a sensitivity of 50% therefore many believe are not accurate for diagnosing CRPS.
What are the denervation level(s) for: Long QT syndrome
Stellate ganglion, G2 and G3

What are the denervation level(s) for: Raynaud syndrome
Stellate ganglion, G2 and G3

What are the denervation level(s) for: Vascular disease
Stellate ganglion, G2 and G3

What are the denervation level(s) for: Complex regional pain syndrome?
Stellate ganglion, G2 and G3

What are the denervation level(s) for: plantar hyperhidrosis?
L2 and L3

What are the denervation level(s) for: facial rubor?
G2

What are the denervation level(s) for: craniofacial hyperhidrosis?
G2

What are the denervation level(s) for: axillary hyperhidrosis?
G4

What are the denervation level(s) for: palmar hyperhidrosis?
G4 or G3

Name 6 rare (< 1%) causes of complications associated with thoracoscopic sympathectomy
- Horner syndrome
- Hemothorax
- Pleural effusions
- Injury to vagus nerve
- Injury to phrenic nerve
- Injury to subclavian artery and vein
Name 4 common causes of complications associated with thoracoscopic sympathectomy
- Compensatory sweating 70-100%
- Segmental atelectasis 1-5%
- Pneumothorax 1-5%
- Subcutaneous emphysema 1-2%

Name 7 secondary IVC tumours that may have tumour thrombus

Name 7 secondary IVC tumours

Name 7 secondary SVC tumours

What is the most common primary tumour of the IVC?
Primary leiomyosarcoma

If you are resecting an IVC tumour and planning to patch angioplasty, how large should the diameter of your patch be?
D x 3 x % of caval wall to be replaced
E.g. IVC 20 mm with 50% resected - 20 x .5 x 3 = 30 mm
