9 - Cutaneous Neoplasms Flashcards
What is seborrhein keratoses? Who gets it?
One of the most common cutaneous neoplasms; delop in middle age or older pts
What is the appearance of seborrheic keratoses?
Brown or tan waxy papules and plaques with “stuck on” or warty appearance.
Commonly on face, trunk, and upper extremeties.
Sudden onset of multiple is associated with internal malignancy, usually stomach cancer (Leser-Trelat sign)

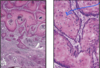
What do you see on histology of seborrheic keratosis?
Pseudohorn cysts

What is actinic keratosis? Who gets it and why?
AKA solar keratosis; common lesions that occur in middle age/elderly population as a result of chronic sun damage.
What is the appearance of actinic keratosis? What is the change of it becoming malignant?
Red or tan/brown macules with “gritty” sandpaper-life scale; some lesions regress or remain stable
0.1-10% become malignant (to become squamous cell carcinoma)

How does actinic keratosis differ from normal skin on histology?
Perakeratosis - retention of nuclei in stratum corneum from increase proliferation.
Granular layer: some loss of granular layer
Jumbled spinous layer
Lower 1/3 of epidermis is irregular

Who commonly gets squamous cell carcinoma? What percent of skin cancers does this make up? What can cause it?
Common in older adults; Makes up 20% of all skin cancers.
Most common cause is UV radiation (DNA damage)
Other predisposing factors: chronic ulcers, old burn scars, HPV, radiation, arsenic, and immunosuppresion.
What is the appearance of SCC in situ? Invasive?
In situ: red scaly plaque
Invasive: lesions tend to be nodular and may ulcerate

What percentage of squamous cell carcinoma (SCC) become invasive? What is a higher risk of metastasis associated with?
5% of in situ develop an invasive component
Risk of mets ~2-4% higher in immunocompromised
Liklihood of mets is related to the location and degree of invation.
How does squamous cell carcinoma differ on histology from normal tissue? What does it look like clinically?
Clinically: thick red scaled plaque
Histology: full thickness atypia - goes from basal layer to the granular layer and you lose the granular layer.

How would you be able to tell that this is invasive squamosu cell carcinoma?

No longer confined to the epidermis; large glassy pink cells.
What is keratoacanthoma? What does it look like?
A variant of SCC; dome shaped pink papule or nodule with central crater keratin plug.

How does keratoacanthoma change over time? What can it cause and who gets it?
Rapidly grows over 2-10 weeks and occurs mainly on sun-damaged skin. Some lesions resolve spontaneously.
Multiple lesions may be present on immunosuppressed.
Can cause extensive local destruction.
What does a keratoacanthoma look like on histology?
Crate-like lesion with well-differentiated proliferating epithelium.
Usually confined to the epidermis.

What is the most common human cancer? What is it caused by?
Basal cell carcinoma - secondary to chronic sun exposire/UV radiation.
Describe the growth of basal cell carcinoma and it’s pattern of metastasis. What defect is it asociated with?
Slow growing tumor that rarely metastasizes. When it does, the patient is often immunocompromised.
Associated with dysregulation of the sonic hedgehog or PTCH pathway (30-40%).
What is the cutaneous appearance of basal cell carcinoma?
Pink pearly papules with prominent arbocing subepidermal blood vessels (telangectasia)
Ulceration and erosion are common.

What is the appearance of nodular basal cell carcinoma on histology?
(nodular is the most common type)
- Blue ball in dermis or budding off of epidermis
- Peripheral palisading
- Retraction: breaks away from surrounding stroma

What is the appearance of acquired melanocytic nevi?
- Pink, tan, or brown
- Uniformly pigmented papules and macules
- Small (usually <0.5 cm)
- Well-defined with smooth borders

What is the difference between sporadic and familial dysplastic nevus syndrome in terms of number of nevi and melanoma risk?
Sporadic: lower number of dysplastic nevi (usually 2-10); lifetime risk of melanoma in the sporadic form is ~10%
Familial: hundreds of dysplastic nevi; lifetime risk of melanoma approaches 100%
**dysplastic nevi, whether familial or sporadic show identical histological features.

What are the histologic features of dysplastic nevi?
Can be junctional or compound
- Lentiginous hyperplasia (prolif. melanocytes)
- Irregular nests
- Bridging of rete ridges (bridging of epidermis)
- Lamella fibroplasmia (of capillary dermis)
- Inflammatory response

What are clinical features of melanoma?
A: asymmetry
B: borders (notched, uneven, blurred)
C: Color (uneven; shades of brown, tan, red, and black)
D: Diameter (>6 mm) - larger than a pencil eraser
E: Evolving - change in color and size

What two things describe melanoma prognostication?
Breslow depth and Clark Level

What is the appearance of mycosis fungoides?
Red or pink scaly patches; stages of patch, plaque, and nodules.
Usually chronic course, although may become aggressive.

Describe mucosis fungoides on histology?
Infiltration of the epidermis and upper dermis by neoplastic T cells, which often have cerebrigorm (folded) nucleus characterized by infolding of the nuclear membrane.
Can also see invasion of blood vessels.
