77/78: Ped Hip, Knee, and Leg - Mahoney Flashcards
(53 cards)
what is the angle of inclination of femur?
- angle in the frontal plane formed by the axis of the head and neck of the femur and shaft of the femur
- Infant-150°
- Adult-125°
- The inclination angle allows abductors to function with a mechanical advantage as they counterbalance body weight in one-legged stance
- w/o –> trendelenburg gait
- Hip abductors should be as far laterally from the hip as possible to achieve muscle stability which is greatest when the child begins to stand

coxa vara vs. coxa valga
-
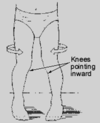
Coxa vara: a decrease in the angle of inclination so that the distal femur is directed towards the midline and the knees are closer together (genu valgum)
- more common
- caused by overgrowth of the femoral epiphysis which leads to limb shortening and limitation of passive hip abduction
-
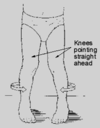
Coxa valga: an increase in the angle of inclination so that the distal femur is directed away from the midline and the knees are farther apart (genu varum)
- uncommon
an abnormal angle of inclination (not achieved the 125) will cause a child to stand with the pelvis tilting down on …
contralateral side
what is alsberg’s angle?
- Alsberg’s angle: angle formed by a line through the epiphyseal plate of the neck of the femur and the long axis of the femur
- Normal adult-41°
- Increase is coxa valga, decrease is coxa vara

what is the normal angle of declination of femur?
- Infant-30° (up to 60°) of internal rotation
- Adult-8° to 12° of internal rotation
- Therefore, angle decreases about 20° (up to 50°) by rotating externally, but still remains internally rotated by about 10° in the adult
what is the angle of declination?
Angle of Declination of Femur: angle in the transverse plane formed by the axis of the neck of the femur and the transcondylar axis of the knee with the apex of the angle lateral when looking from proximal to distal through the femur

why is normal fetal position described “buddha”
hips and knees flexed, hips externally rotated, legs and feet internally rotated
- When the HIP is flexed in utero, it is also externally rotated
- When the LOWER LIMB is flexed in utero, it is also internally rotated
version vs. torsion
- both refer to how much twist is in the bone
-
Version: angular difference between the transverse axis of motion of each end of a long bone (does NOT mean soft tissue position) normal
- Normal version is present when the angular difference is within 2 standard deviations of the mean
-
Torsion: present when the version is excessive (abnormal) or greater than 2 standard deviations outside of the mean
- clinically = deformity or abnormality
femoral antetorsion
- medial femoral or internal femoral torsion-abnormal increase in femoral anteversion
- Retrotorsion: lateral femoral or external femoral torsion-abnormal increase in femoral retroversion
femoral vs. tibial version
- Femoral version: angular difference between the transcondylar axis of the knee and the neck of the femur
- Tibial version: angular difference between the transcondylar axis of the knee and the transmalleolar axis of the ankle
When looking at our diagram, the axis of the neck of femur makes a larger angle with the transcondylar axis of the knee =

- answer = Femoral anteversion: the normal angle of femoral version made when the axis of the neck is directed forward or anterior from the femoral shaft
- Femoral retroversion: the angle of femoral version made when the axis of the neck is directed backward or posterior from the femoral shaft
- When looking at our diagram, the axis of the neck makes a smaller angle with the transcondylar axis of the knee

A femur which exhibits an internal rotation less than 2 standard deviations from normal is called
femoral anteversion
- Femoral torsion: abnormal increase in femoral version
- Antetorsion: medial or internal femoral torsion-abnormal increase in femoral anteversion
- Retrotorsion: lateral or external femoral torsion-abnormal increase in femoral retroversion
- At birth the femur is rotated internally to about 30°
- At the same time, the soft tissue of the hip externally rotates the thigh to about 50°
how does this change as you age?
- The angle of declination decreases from 30° internal to about 10° internal (or femur externally rotates 20°)
- Subsequently, the soft tissue changes around the hip, internally rotate thigh from 50° external to 10° external (or internally rotates thigh 40°)
- The 8 to 12° of femoral anteversion is balanced by the external rotation of about 10° caused by normal soft tissue contraction at the hip
- The end result is that the knee is eventually pointed straight ahead in gait (by 4 years of age)
normal hip rotational development
- Infants: 60-90° external; 0-30° internal (3:1 ratio)
- Up to 1 year: 50-60° external; 30° internal (2:1 ratio)
- 4 years to adult: 45° external; 45° internal (1:1 ratio)
- When this does not occur, we will have either an externally rotated or internally rotated leg and foot
osseous antetorsion will cause an … gait
osseous retrotorsion will cause an …. gait
_*******_
- Antetorsion will cause an in-toe gait, retrotorsion an out-toe gait
- An in-toe gait can also be caused by tightness of the internal rotators of the hip or a tight iliofemoral, pubofemoral, or ligamentum teres ligament
- An out-toe gait can be caused by tightness of the external rotators of the hip or a tight ischiofemoral ligament
muscles that are external hip rotators
gluteus maximus
obdurators
adductors
gemelli
sartorius
quadratus femoris
piriformis
muscles that are internal hip rotators
gluteus medius
gluteus minimus
How do we determine if the rotational deformity is due to femoral torsion or a soft tissue contracture (or laxity)?
- Need to determine neutral femoral position of the hip with the hip extended and with the hip flexed
- A difference between NFP readings with the HF and HE suggests that there is a soft tissue cause of the rotational deformity
- The same reading for NFP with the HF and HE suggests it is solely femoral torsion
A 2 year old child presents with an out-toe gait. You measure 60° of external hip rotation and 40° of internal hip rotation with the hip flexed and extended. is this normal?
yes, it is femoral retroversion
if this was a 6 yo = femoral retrotorsion
describe the uterine position
- This uterine position leads to:
- an increase in external rotation and flexion of the hip
- femoral anteversion caused by femoral head and neck rotating inward against the shaft-allows maximal rotation of hip in flexed position
- The anteverted hip fits well into the acetabulum in utero while the hip is hyperflexed (walking on all fours is the true physiologic position of the hip), but as soon as the hip extension begins after birth, anterversion angle must be reduced or there will be an unstable, ANTERIOR dislocatable hip or an in-toe gait
- Anteverted position increases leverage of the gluteus maximus which allows it to better maintain the body in an upright position
- However, the upright position on an anteverted leg causes the anterio-superior portion of the femoral head to be exposed
the anteverted position of the femur is important because …
- It is the most stable position of the hip in utero
- It allows the child to walk in-toed which is more stable
- It increases the leverage of the gluteus maximus
- It increases the leverage of gluteus medius and minimus
1 and 3
what 3 activities occur to mold the epiphysis of the femoral head to reduce anteversion?
- Upper end of femur yields under pressure to tight anterior capsule so that excessive anteversion slowly molded away
- Torsion at birth is reduced when the erect posture is assumed by pressure on the tense anterior hip capsule
- Major force
- if anterior capsule stretched, the hip dislocates anteriorly. Less force is exerted on the femur, so there is less tendency for correction of anterversion
- Force also produced by contraction of internal rotator muscles and external rotators which gives rise to a shearing force acting in the AP direction on the femoral head which causes the femoral epiphysis to slip and reduce anteversion
- Pelvic movement of inward rotation on a loaded hip joint also applies a dynamic force in the AP direction on the femoral head
* therefore …. walking is the decisive factor for reducing anteversion (as well as, the angle of inclination)*
Leads to an intoe gait, anterior pelvic tilt (to cover the femoral head), lumbar lordosis, apparent genu valgum (due to internal positioning of the patella), genu recurvatum, and possible flatfoot to compensate for foot adduction (causes skewfoot)
femoral antetorsion
most common cause of intoeing after age 2/3
- internal femoral torsion or antetorsion or tight internal hip rorators and/or tight iliofemoral, pubofemoral or ligamentum teres ligaments
- The most common cause of outoeing at any age is external femoral torsion or retrotorsion or tightness of the external hip rotators and/or ischiofemoral ligament