Psychobiology and motivation (year two) Flashcards
Name the 5 major structures in the brain
- Myelencephalon: medulla, comprises tract between brain and spinal cord
o hindbrain - Metencephalon: pons and cerebellum
o hindbrain - Mesencephalon: thalamus and hypothalamus
o midbrain - Diencephalon: thalamus and hypothalamus
o forebrain - Telencephalon: cerebral cortex, limbic system, basal ganglia
o Forebrain
Describe the composition of the cerebral cortex
- Made of grey matter – small unmyelinated neurons
- White matter= large myelinated axons
- Convolutions – increase surface area
o Large – fissures
o Small – sulci
o Ridges between fissures and sulci – gyri - Longitudinal fissure separates hemispheres (connected by cerebral commissure, incl corpus callosum
- Contains neocortex and subcortical structures (hippocampus, limbic system, basal ganglia)
Describe the composition of the neocortex
- Newest part of cerebral cortex
- Neocortex = largest part of cerebral cortex (90%), other 10% is allocortex (cont hippocampus)
- Six layers
- Large neocortex ratio, correlates with complexity of behaviour
- Central/lateral fissure divide each hemispheres into 4 lobes
Give the neocortex lobes and state their functions
- Frontal lobe: motor cortex (precentral gyrus)
o Complex cognition in frontal cortex - Parietal lobe: (post central gyrus)
o Somatic sensations, orientation, object location - Temporal lobe: hearing and language
o Complex visual patterns
o Memory - Occipital lobe: visual processing
Explain the origins of phrenology
- Franz Joseph Gall (1758-1828) founded phrenology
- Tried to make assumptions about intellect and personality from examination of skull shape - assumed surface of skull reflected regions of brain development
- Classmate could recite long passages of prose and had bulging eyes – assumed that verbal memory lay in frontal region behind eyes
- Lectures on crainioscopy offended religious leaders and was banned in 1802 by Austrian government
- Identified 27 cranial regions that corresponded to traits
- Found regions responsible for murder/inclination to steal (felt criminals heads to detect patterns
Give some of the positive contributions of phrenology to modern day psychology
o Believed brain was physical organ of the mind
o Proposed that cerebral cortex contains localised function areas (proved right, broca’s area and motor cortex)
o First to identify grey matter with neurons and white matter conducting tissue (ganglia)
Describe how lesion studies led to the discovery of Broca’s aphasia
- Broca consulted about patient with neurological issues and no speech
- Could only say word “tan”
- Autopsy revealed left frontal lobe lesion
- Second patient: stroke patient, could only say 5 words
o Same lesion as Tan
o Known as Broca’s aphasia: inferior frontal gyrus on left cerebral hemisphere
Describe how lesion studies led to the discovery of Wernicke’s aphasia
- Broca: damage to Broca’s area should disrupt production, not comprehension
- Wernicke: lesions to Wernicke’s area produce primarily receptive syndromes
o Wernicke’s aphasia: poor written and spoken language comprehension, meaningless speech, speech still retains structure/rhythm/intonation
o “Word salad”
o Left temporal lobe
Explain what Brodmann areas are and how they are organised
- German neurologist Korbinian Brodmann (1868 – 1918)
- Produced maps of train based on cytoarchitectural organisation of neurons in CC (using nissl method of cell staining)
- Identified 52 areas of cerebral cortex differing histologically (cells/structures) – Brodmann’s areas
- Defined solely on neuronal organisation – since been correlate to diverse cortical functions
- Provided map based on collections on neuron types – examined using lesion studies, experimental ablation, functional neuroimaging
Define functional neuroanatomy
- Moved from basic naming of lobes to naming areas by function e.g motor areas, visual cortex
- General classification of three functional areas: sensory, motor and association
Describe the functions of the prefrontal cortex
- Very developed in humans
- Belies complex cognition, thought, social behaviour, personality etc
- Executive functions: higher order cognitive functions – word fluency, inhibition, switching attention
- Working memory
- Recall
Explain the implications of prefrontal cortex damage
- Early studies: large portions of PFC can be removed without loss of mental capacity – gave revise to development of lobotomy/leucotomy
- Lobotomy: severing connections from PFC to other brain areas
- Procedure introduced by Antonio Egas Moniz – won nobel prize for medicine for discovering lobotomy as a treatment for psychosis
- Mixed success: some patients more docile, others committed suicide or were severely brain damaged
- David Ferrier (1876): ablation of frontal lobes in monkeys resulted in loss of faculty of attentive and intelligent observation but senses unimpaired
Give the subdivisions of the prefrontal cortex and their functions
- Dorsolateral PFC: working memory, rule-learning, planning
- Orbitofrontal PFC: inhibitory/emotional control and inability to function in social domains
- Ventrolateral PFC: human inferior temporal gyrus, disparate functions - spatial attention, inhibitory control, language
Describe the role of the primary motor cortex and what led to its discovery
- Precentral gyrus
- 1937: Penfield and Boldrey mapped primary motor cortex of conscious human patients during neurosurgery with electrical stims on cortical surface (noted which body parts moved in response to stimulation)
- Each stimulation activated a contralateral muscle and produced simple movement – primary motor cortex is organised somatotropically
- Somatotopic layout referred to as motor homunculus
Describe the implications of lesions to the primary motor cortex
- Extensive damage to PMC doesn’t eliminate all voluntary movement
- Large lesions to PMC disrupts ability to move individual body parts independently, reduces speed/accuracy/force
- Other movements able due to association and secondary motor areas
Describe the role of association motor areas
- Posterior parietal association cortex: integrates orientation info about body parts/external objects positions
- DLPFC receives projections from posterior parietal cortex and projects to secondary motor cortex, primary motor cortex and frontal eye field
- DLPFC responds in anticipation of motor activity
Describe the role of the secondary motor cortex and explain how it processes information
- Receives input from association cortex
- Premotor cortex:
o Anterior to primary motor cortex
o Receives highly processed sensory info
o Planning of movement - Frontal eye field
o Anterior to premotor cortex
o Controls voluntary eye movements - Electrical stim of secondary motor area elicits complex movements, involving both sides of body
Describe the role of sensory areas and what they consist of
- Consist of primary, secondary and association areas
o Primary areas receive input from thalamic relay nuclei
o Secondary cortex receives input from PSC or other secondary areas
o Association areas integrate info from more than one sensory system - Posterior parts of brain behind central sulcus
- Large parts of brain dedicated to processing sensory stimuli
- Postcentral gyrus = location of PSC
Describe the role of the primary somatosensory cortex
- Penfield et al. (1937) – electrical stim to cortical surface (conscious patients)
- Brodmann areas 1-3 (in postcentral gyrus) – sensations in various areas
- Somatotropic organisation
- Medial parts = leg, lateral parts = face – more sensitive to touch
- Distribution biased towards areas with high sensory discrimination e.g fingers, mouth
- SII (secondary somatosensory cortex): ventral to PSC in postcentral gyrus – receives input from PSC
Explain the implications of damage to the somatosensory system and association cortex
- Damage to PSC has mild effects
- Corkin et al (1970) – unilateral lesion of PSC in epileptics – two minor contralateral deficits – ability to detect light touch, reduced ability to identify objects by touch
- Somatosensory signals conducted to highest level of sensory hierarchy is association cortex
Describe the role of the visual cortex
- Vision represented in brain in three main regions
- Primary visual cortex: posterior occipital lobe
o Most input from visual relay of thalamus - Secondary visual cortex (prestriate and inferotemporal cortices) : receive input from PVC and visual association cortex
- Association cortex: posterior parietal cortex
Explain the implications of damage to the primary visual cortex
- Produces a scotoma (area of blindness) in corresponding area of contralateral visual field
o Contralateral = side of body that is opposite to that of the brain structure - Many patients unaware of scotomas – visual completion occurs
Give the areas of the visual system
- 12 functional areas of VC identified
- About 30 in monkeys (24 secondary, 7 association)
- Selective lesions produce different visual losses
Define and locate the dorsal and ventral streams
- Info from PVC projects to areas of SVC and AC by dorsal and ventral stream
o Dorsal stream: projecting up to posterior parietal cortex
Spatial stimuli (location of objects, movement)
o Ventral stream: projects across to inferotemporal cortex
Characteristics of object (colour, shape)
Describe what deficits can result from damage to the dorsal and ventral streams
- Damage to posterior PC – can describe objects but can’t touch them
- Damage to ITC – difficulty describing, but can pick them up
Describe what can happen if there is damage to the secondary visual cortex
- Prosopagnosia (face blindness)
- Coined in 1947 by Joachim Bodamer
- Usually results from damage to right fusiform gyrus during head trauma/stroke/degenerative diseases
Give examples of sensory areas and their Brodmann areas
- Auditory areas – primary auditory cortex: superior temporal lobe, inside lateral sulcus (BA 41)
o Auditory association area: posterior to PVC (BA22) – evaluates sounds - Gustatory (taste) cortex – BA43, roof of lateral sulcus
- Olfactory cortex – medial temporal lobe, connects to limbic system
- Association areas are where primary inputs are processed/comprehended
Define and explain the role of monoamine pathways
- Neurotransmitter pathways have been mapped
- Dahlstrom and fuxe (1964) – used immunofluorescence staining to visualise pathways of serotonin, dopamine and noradrenaline
- MN emanate from brainstem and project to forebrain and beyond
Define and explain central lateralisation of function
- Left/right cerebral hemispheres separated apart by cerebral comissures
- Dax (1836) – 40 brain damage patients had speech problems and damage in left hemisphere
- FMRI, PET, unilateral lesions, split brain patients studied
o Language/motor abilities of left hemisphere apparent
o No substantial differentces between hemispheres, may only have slight biases - Lateralisation is statistical – language is most lateralised
- Some skills show hemispheric dominance
Describe and explain how functional MRIs work
- Shows structure and activity of brain
- Blood flow are neuronal activation coupled
- FMRI detects changes in blood flow due to blood being diamagnetic
- Laird et al. (2009) Extensive convergence in large portions of left inferior frontal gyrus, centering on BA 44/45 (Broca’s area)
Define and explain functional connectivity analysis
- fMRI analysis technique to observe which brain areas correlate with another in terms of activation
- Can measure BOLD signal from entire brain during task encompassing the reward system and compare to relevant groups
- Can examine BOLD signal changes associated with the trains when we expect system level activation
Describe how technology is advancing frontiers in neuroscience
- Transcranial stimulation: non-invasive method of brain stimulation
o Relies on electromagnetic induction using insulated coil placed over the scalp
o Focused on area of the brain thought to play role in mood regulation - Brain computer interface: can help those with paralysis of the body to communicate using electrical signals from their brains
Define morphology
Morphology: classification in terms of number of neuronal processes (projections from cells)
Give two types of multipolar neurons
Two types of multipolar neurons
Golgi 1 neurons: long axons
Golgi 2 neurons: shorter axons, project locally
Give the three major purposes and types of neurons
Three major purposed:
Sensation – afferent neurons
Gather/send info from senses
Integration – interneurons
Process all info gathered
Action – motor neurons
Send signals to effectors e.g muscles and glands
Give a definition of pain
“An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” – International Association for the Study of Pain (2020)
Give the three dimensions of pain
Dimensions of pain:
Sensory: physical stimulus, intensity, location
Affective: unpleasantness, emotions
Cognitive: attention memory, expectation, imagination
Explain sensory integration
From receptors to spinal cord to brain
Transmitted via primary sensory neurons (nociceptors) – spinal cord – streamed up to CNS via multipolar neurons (golgi 1 type)
Describe projection neurons
Projection neurons: project from spinal cord to the brain
Define nociceptive-specific neurons
interneuron specialised for processing pain
Define Wide-dynamic range neurons
interneuron specialised for dealing with painful and non-painful stimuli
Define descending pathways
Descending pathways: neurons descending from brain to spinal cord to modulate pain in SC, dictates pain sensitivity
Explain how nociceptive processing is arranged in the central nervous system
Nociceptive processing in CNS is distributed and degenerate
See Coghill R
Distributed: processing is done independently by multiple sites in CNS, multiple brain regions activated in parallel
Degenerate: have a very resistant pain response system: there is no single brain centre. Not one area of the brain can be disturbed and completely stop pain sensation
Multiple brain areas dedicated to pain, all with the same function
Describe the role of sensory neurons
Contains receptors (either cellular e.g vision, molecular e.g pain)
Translate receptor codes to neural codes
Transmit information to CNS
E.g visual neuron: bipolar, attached to cellular receptor (cilia sensitive to physical stimuli of light)
E.g of cellular receptor: rods and cones
Describe the anatomy of nociceptors
Nociceptors (pain sensors) are free nerve endings
Epidermis doesn’t contain nociceptors
Nociceptors contained in dermis
Describe the anatomy of the epidermis
Epidermis doesn’t contain nociceptors
Nociceptors contained in dermis
Merkel discs and Meissner discs: cellular receptors at end of touch fibres, detect different subtle types of pressure
Molecular receptors: small compared to cellular receptors, polymodal (detect many types of pain e.g pain by pressure, chemical pain – chilli from capsaicin, temperature)
Describe the role of TRP channels
TRP channels: most common type of molecular receptor for pain
Voltage gated calcium channels
Describe the role of the TRP V1 channel
TRP V1 channel let calcium into cell from outside, triggering change in membrane voltage generating action potential
Agonists: temperatures above 43’, capsaicin, anandamide (found in chocolate and plants, fatty acid neurotransmitter), acid environments, osmotic pressure
Define conformational change
Conformational change: change in protein structure allowing calcium ions to enter into cell, depolarising the membrane and generating action potentials
Describe the anatomy and role of C fibres
C fibres:
non-mylinated
carry mechanical, thermal and chemical pain
- 2-1.5 mm diameter
- 5-2m/s conduction speed (walking)
Describe the anatomy and role of A-Delta fibres
A-delta
Mechanical and thermal pain
Myelinated
1-5 mm diameter
5-40 m/s conduction speed (cycling)
Describe the anatomy and role of A-beta fibres
A-beta
Touch information
Myelinated
6-12 mm diameter
35-90 m/s conduction speed (race car)
Describe the anatomy and role of A-Alpha fibres
A-Alpha
Proprioception
Myelinated
13-20mm diameter
80-120 m/s conduction speed (jet plane)
Explain which fibres and responsible for first pain
A-delta fibres responsible for first sensation of pain, C fibres responsible for slower, aching pain
First pain sensation takes 2-300ms
Explain which fibres are responsible for second pain
Second pain sensations take 1 second to reach the brain, longer duration
EEG: c fibre has lower amplitude and is harder to measure on EEG
First pain encoded partly within somatosensory cortex, second pain encoded in anterior cingulate cortex and posterior insula cortex
Describe the nociceptive pathway in the spinal cord
Peripheral sensory neurons have cell bodies in dorsal root ganglion (unipolar neurons), axons continue into dorsal horn and synapse on various interneurons or projection neurons (these cross spinal cords and enter spinothalamic tracts – goes to brain)
10 laminae in spinal cord: different types of cells, including different types of neurons
Describe where substantia gelatinosa and WDR interneurons are found
Substantia gelatinosa interneurons
Mainly found in laminar 2
Wide dynamic range interneurons
Mainly found in laminar 5 and 3
Explain the gate control theory
Important for gate control theory
Non-painful sensory inputs close the “gates” to painful input, reducing pain
SG neurons of dorsal horn are inhibitory
C fibres (pain) inhibit SG neurons
Ab-fibres (touch) excite SG neurons
SG acts as gate and determines whether pain is encoded within WDR neurons that transmit info to brain
Explain the population coding theory
Population coding theory
Recruitment of larger numbers of WDR neurons is associated with increasing intensities of pain
Relationship between WDR neurons and pain could be due to WDR neurons having larger receptive fields (provides mechanism for spatial summation of pain)
WDR neurons selectively expand receptive fields in response to nociceptive inputs
Increasingly intense noxious inputs increase size of RFs – more WDR neurons activated by more intense stimuli
Noxious stimulus intensity can be encoded by progressive recruitment of increasing WDR neurons
Noxious inputs = pain inputs
Explain spinal integration
Spinal distribution of nociceptive input/ potential neuron recruitment may be driven by widely branching primary afferents and propriospinal interconnections
Primary afferents (A-delta and C-fibres) branch before entering spinal cord
Activation of ascending neurons in segment
Activation of ascending neurons in a different segment
Propriospinal interconnections may transmit nociceptive information, even to contralateral dorsal horn
Propriospinal interconnections provide substrate for wide ranging facilitation/inhibition of neurons across many spinal segments
Explain lateral inhibition
Spatial perception sharpened due to inhibitory integration process
Also explains nonlinearity of spatial summation of pain i.e stimuli that are close together summate less than those further apart (up to about 20cm)
Explain and define pain pathways
1st neuron: spinal ganglion – grey matter of spinal cord
2nd neuron (projection neuron, excitatory): grey matter – thalamus, crossing in anterior part of spinal cord
3rd neuron: thalamus (ventrobasal complex) – multiple brain areas of cerebral cortex activated parallel
Somatosensory cortex, posterior insula, anterior cingulate cortex , amygdala
Amygdala can be activated by parabrachial nucleus which bypasses the thalamus, can be activated earlier
All send info in a descending fashion, back down via the amygdala into the brain stem, first to periaqueductal gray then to rostral ventromedial medulla (involved in descending modulation of spinal cord)
Spinothalamic tract (anterolateral system)
Explain and define descending nociceptive control
Endogenous opioid-mediated
These are primary neurotransmitter by which insula, ACC, amygdala and hypothalamus communicate with brain stem
Info is send to first region in brain stem within midbrain – contains nucleus called periaqueductal gray
Info then sent from PAG to medulla, containing rostral ventromedial medulla
Midbrain and medulla work together and act like computer system
PAG like computer which receives info from cortical regions via endogenous opioid system then weighs up info and decides how much inhibition to apply to spinal cord
This weighing up is then sent to medulla, which acts as executer – executes instructions from PAG
Switches from opioid system to serotonin system and sends descending projections down long neurons (up to 1m) and NT now involved is serotonin
Give evidence for descending nociceptive control
Electrical stim of PAG/RVM causes behavioural suppression to pain response (Reynolds, 1969)
Microinjections of morphine opioid receptor agonist has the same antinociceptive effect
Explain research findings on investigating the integraity of neuroanatomy following potential insults due to heavy drug use
Ecstasy/MDMA produces effects by stimulating release of serotonin
Increases in serotonin neurotransmission following MDMA use is produced by action at serotonin transporter (SERT)
Can measure integrity of serotonin is PET and SPECT scans
Use makers for pre/postsynaptic serotonin
Participants injected with radioligand – radioactive tracer that will bind to SERTS or postsynaptic 5-HT neurons
Studies compare regular ecstasy users to controls (no ecstasy use)
Data meta-analysed over all studies
RESULTS
Ecstasy users showed significant SERT reductions in 11/14 brain regions, including every neocortex/limbic region
LIMITATIONS
7 Studies, low statistical power
Could not do meta regression to correlate drug use with SERT data
Use of other drugs cofound – few people use only ecstasy (ends up being drug users vs nondrug users)
Cannot say anything about reversibility of effects
Self-report issues
No data on actual cognitive function
No report on purity of the ecstasy taken – only know crude mention of ecstasy taken
Could assume effects were due to ecstasy as no known effect of cannabis on serotonin, but would be a guess
Explain research findings of regular cannabis use on neuroanatomy
Regular cannabis use associated with comorbid psychopathologies, higher levels of depression, anxiety, psychosis, deficits in performance in areas of cognition incl reward processing, learning and memory
SMRI
Regular exposure to cannabis (ongoing use and up to 28-day abstinence)
Reduced hippocampus volumes compared to controls – involved in memory
Reduced orbitofrontal cortex volumes – reward processes thought t be relevant in aetiology of substance dependence – motivation and reward functions
LIMITATIONS
Small statistical volumetric group differences – considerable overlap between regular cannabis users and controls
Neural differences between cannabis users and controls may normalise with prolonged abstinence
Cannabinoid compounds encapsulated in commonly smoked cannabis may exert independent/interactive effects
Define degeneracy
Lack of specialisation
Multiple brain areas responsive to pain
Even if anterior cingulate cortex is removed (as tried in history) pain does not cease
Damage to an area of spinal cord does not completely cause loss of pain sensation
Neuropathic pain: can increase the pain you feel, caused by damage to nerves
Difficulty to feel non-noxious sensations e.g vibration
Explain which integrative neurons are responsible for the perception of pain intensity. Include research findings in your answer
substantia gelatinosa interneurons
gate neurons
mediate between touch sensation and pain sensation
wide dynamic range neurons
original article: Coghill, R.C et al (1993) – gerbil strangler
would apply different temperature plates to rats
pain threshold for temperature on skin: 49’C is moderate to high temperature
would disconnect brain from spinal cord before studying spinal cord – modulation complicates data
peripheral nociceptors innovate L4 (region of spinal cord) at 45’C – activate of wide dynamic range neurons
WDR neuron activate in area L2-L5 at 49’C
Give evidence for wide dynamic range receptive fields
EVIDENCE: WDR receptive fields
Expansion of WDR receptive fields
Original article: Cook, A.J et al (1987)
20 second electrical stimulus applied to brain (low to high intensity)
Low receptive field for low intensity (just toes)
High receptive field for high intensity (whole leg) - more WDR neurons activated
Give evidence for spatial summation
EVIDENCE: spatial summation
Large receptive fields of WDR neurons support spatial summation, since the same neuron can respond to stimuli at 2 different locations
Can occur even when stimuli are separated by 40cm in humans
But, maximal at 55- and 10-cm separation distances (smaller distances summate less – due to lateral inhibition)
Original article: Quevado, A.S. and Coghill, R.C (2009)
Explain whether you need a brain to respond to pain
withdrawal reflex
sensation can be modulated by expectation
attention modulates spatial summation
when participants were instructed to provide an overall rating of 2 noxious stimuli, substantial spatial summation of pain was detected
caused by top-down modulation of spine
attention modulates spinal nociception
neuronal responses to painful stimulation in dorsal horn were significantly reduced under high WM load
reductions of spinal responses correlated with distraction from pain effect: reduced pain perception by distraction
likely to involve both opioidergic and nonopioidogenic – opioid antagonist did not completely block the anti-nociceptive effect of distraction
regions of anterior cingulate cortex have projections in laminae V-VII (including WDR neurons) – may provide attentional information to spinal neurons
ability to distract from pain can be life-saving e.g during war
Describe the role of PAG, RVM AND DLPT in descending nociception
PAG calculates how much analgesia to apply from opioidergic inputs from multiple brain regions
RVM and dorsolateral pontine tegmentum (DLPT) – exerts anti-nociceptive effect via serotonergic projections down to spinal cord
When you get hurt – and it’s not a serious injury – you instinctively start to rub the affected area or start shaking it vigorously. Which types of interneurons do you think might be involved?•
Theory: Gate Control Theory of Pain
C-fibres inhibit and Ab-fibres excite substantia gelatinosa (SG) of the dorsal horn
The SG consists of inhibitory interneurons that act as the gate and determine which signals should reach the WDR cells and then go further through the spinothalamic tract to reach the brain
Substantia gelatinosa (SG) neurons:–Multipolar - short axons–Spinal cord – lamina II–Inhibitory interneuron–GABA neurotransmission
Other relevant neurons:–WDR neurons: Multipolar with long axons; Spinal lamina V; Excitatory ascending projection neurons; Glutamate.–Peripheral nociceptors (e.g. C-fibres): Pseudo-unipolar; DRG (cell body); Excitatory; Glutamate.
Explain the therapeutic implications of gate control theory
TENS (transcutaneous electrical nerve stimulation)
Trains of high-frequency electrical stimuli, applied to the skin (nerve), attenuate pain for minutes or hours
Explain how spinal cord stimulation can help neuropathic pain
Stimulation of the dorsal horn tract system alleviates chronic pain: therapy by direct or epidural electrical simulation of the spinal cord
Article: Stancak et al., Eur.J.Pain (2008)
Explain how sensory adaptation occurs in context change
Exposure to bright light: pupils constrict and photoreceptors become less sensitive – stops you becoming overwhelmed
Eating fruit after chocolate cake – being underwhelmed
Explain peripheral adaptation
Peripheral adaptation: reduces amount of info that reaches CNS
Level of receptor activity changes – receptor responds strongly at first then gradually declines e.g change in retina, inner ear muscles
Explain central adaptation
Central adaptation: at subconscious level, further changes the amount of detail arriving at the cerebral cortex
Along sensory pathways in CNS
Involved inhibition of neurons along a sensory pathway e.g spinal cord, brainstem
Gradual decrease in the neuronal response of the sensory system, over time in response to a constant stimulus
Give examples of central adaptation
Sharpening: enhancing discrimination
Exposure to a complex stimulus can increase the ability to discriminate its features over time
Maintaining perceptual constancy: invariant percepts despite varying contexts e.g colour constancy
Highlighting novelty:
Detecting and responding to novel events is crucial for survival in a rapidly changing environment
Frees up attention/resources to attend to other stimuli
Efficient coding:
So that neural resources are not wasted on expected properties of the stimulus and can be devoted to signally unexpected stimuli
Explain predictive coding
As a compression tool
Linear predictive coding used since 50s to compress audio speech patterns for better transmission
As a general mechanism of perception
Efficiency is important for brain to minimise energy expenditure (20% of body total energy)
Accounts for some properties of extra classical receptive fields in dorsal ventral stream e.g sharpening
Give the symptoms of complex region pain syndrome
Symptoms:
Intense/exaggerated pain
Hypersensitivity to touch, hot/cold
Fluctuated swelling
Changes in skin colour/temperature
Changes in sweating/nail/hair growth
Pathophysiology is complex and varies
Range of biomarkers needed to support patient stratification/improve diagnosis certainty
Give some neuropsychological markers of CRPS
Increased 2-point discrimination threshold: stimulates two close together places on the skin
Digit identification: 48% of CRPS patients impaired for accuracy (Forderreuther et al., 2004)
85% patients impaired for accuracy OR response time (Kuttikat et al., 2017)
Stereognosis: identifying objects
Hand laterality recognition: identifying left or right hand
Give hypotheses of how integration contributes to CRPS
Theory: problems with spatio-temporal integration contribute to CRPS
Possibilities
Deficit in bottom-up adaptation – would increase overall response to spatially repetitive stimuli over time
Deficit in top-down adaptation – would increase responses to spatially rare stimuli over time
Explain the predictive coding model
Brain tries to predict sensory inputs; must contain representations of input probabilities
Larger mismatch responses thought to be prediction errors
Give the conclusions of Brown et al.
Larger “prediction error” like signal in CRPS patients
Results consistent with inefficient predictive coding in CRPS patients
Suggests deficit in top-down central neuronal adaptation
.Describe how postsynaptic potentials are generated
Postsynaptic cell membrane is polarised – resting-potential of approx. -70mv
NTs in synaptic cleft bind to receptors 9on the postsynaptic membrane and open channels
This allows sodium/potassium/chloride/calcium ions to enter cells – changes degree of positive or negative charge inside cell
Explain hyperpolarisation and depolarisation
Adding +/- ions can:
a. Positive ions increase likelihood signal will be sent by neuron
i. By making charge on PS membrane more positive e.g 70mv to 67mv
ii. Depolarises neuron
iii. Called excitatory postsynaptic potentials
b. Negative ions make it less likely that signal will be sent
i. By making charge on the PSM more negative e.g -70mv to -72mv
ii. Hyperpolarises neuron
iii. Called inhibitory postsynaptic potentials
Define graded in terms of PSPs
Change in post-synaptic potential is graded
a. Stronger signals from neurons result in greater depolarisation or hyperpolarisation
Explain how postsynaptic potentials are conducted
1Potential conducts passively from site of origin
- Conduction of PSPs have 2 important characteristics:
o Rapid – instantaneous
o Decremental – get smaller as they travel
- PSPs do not travel more than a few mm from site of generation before degrading
Describe how integration of PSPs works
- Typical postsynaptic neuron receives signals from many presynaptic neurons at the same time
- Balance between excitatory/inhibitory PSPs determines whether action potential fires
- Integration = combining number of signals into one signal
- Threshold of excitement: usually -55mV
o If net sum of signals reaching axon initial segment (next to axon hillock) depolarises membrane to this level, then an action potential will fire
Define temporal and spatial summation
Spatial summation : integrating incoming signals over space
- Temporal summation: integrating incoming signals over time
Explain why an action potential fires
If integration of PSPs conducts/surpasses threshold of excitation at the axonal hillock – action potential will fire
Describe action potentials
Action potential
o Membrane potential is reversed (negative to positive)
o Very quick (1msec)
o All or none response
Describe the moving of ions from resting potential to hyperpolarisation
Resting potential: voltage gated ion channels closed
- Depolarisation: Sodium channels open, rapid influx of Na+ into cell
- Peak: Na+ channels begin to close, K+ channels open
- Repolarization: Na+ stops entering cell, K+ ions move out
- Hyperpolarisation: K+ channels start to close but some K+ ions continue to move out
Define refractory period and the types of RP
Potential after signal has been sent
- Absolute refractory period: brief period, impossible to generate an action potential
- Relative refractory period: higher than normal levels of stimulation required to generate action potential
Define refractory period and the types of RP
Potential after signal has been sent
- Absolute refractory period: brief period, impossible to generate an action potential
- Relative refractory period: higher than normal levels of stimulation required to generate action potential
Explain how refractory periods are responsible for direction of travel and rate of firing
RESPONSIBLE FOR:
o Direction of travel – soma to axon
Prevents action potential from travelling backwards
o Rate of firing – indicating strength of stimulus
Strong stimulus allows neuron to fire after absolute refractory period
Weak stimulus will note generate action potential until after relative refractory period
Describe and explain propagation
APs travel along axon depolarizing as it goes
- In grey matter – active process: none-decremental
- As with AP generation, conduction of AP along the axon occurs due to influx of sodium – requires opening of sodium channels
Explain how action potential conduction changes when axons are myelinated
Aps travel faster in white matter – axons myelinated
- Saltatory conduction: within myelination sections of axon the signal is conducted passively (decrementally) without needing the opening of channels – augmenting effect on efficiency and speed of transmission
Give the two types of neurotransmitters
Small molecule NTs
o Few components e.g single amine components/ short chains (amino acids)
2. Large molecule NTs
o Contain between 3-36 amino acid molecules
o Often known as neuropeptides
o 100+ identified, categorised into functional groups e.g pituitary peptides, opioids, brain-gut peptides
Define monoamines and describe the two types, giving examples
Singular components
- Catecholamines:
o Dopamine
o Norepinephrine
o Epinephrine
- Indolamines
o Serotonin (5H-HT) 5-hyproxytryptamine
Explain how dopamine and serotonin can be modulatory
Modulatory NTs: can be both excitatory and inhibitory – varies by receptor
o At least 5 dopamine subtype receptors
o At least 14 serotonin receptor types
- Prevalence of receptors with varying functions can form pathways
Give some of the major dopaminergic pathways and their functions
VTA = Ventral tegmental area
- Nigrostriatal: substantia nigra → striatum (motor control/movement)
- Mesolimbic: VTA → Limbic system (reward/reinforcement – addiction)
- Mesocortical: VTA → prefrontal cortex (working memory, planning)
- Tuberoinfundibular tract (hypothalamus → pituitary) (neuroendocrine regulation
Give some of the major serotonergic pathways and their functions
Dorsal raphe nuclei → cortex, striatum
- Medial raphe nuclei → cortex, hippocampus
- Roles in:
o Mood
o Eating
o Sleep/dreaming
o Arousal
o Pain
o Aggression
- Define Ex-vivo and give some en-vivo imaging techniques
Ex-vivo: after death
- En-vivo:
o Contrast x-rays (cerebral angiography)
o Computer tomography (CT)
o MRI
o PET
- Give the basics of MRI
- Strong magnetic field cases H atoms to align by orientation – lattice structure
- Radio frequency pulse passed through scanner
o Atomic nuclei emit EM energy - Scanner detects energy radiated from each spatial location in the chamber
- Computer reconstruction image a 3D model
- Advantages
o No ionizing radiation exposure
o Excellent spatial resolution - Disadvantages
o Cost
o No ferrous metals
- Describe the hardware of MRI machines
- MRI magnet is supercooled by liquid helium – very powerful and expensive
- 60,000X Earth’s magnetic field
- Describe how Structural MRIs work
- Records a signal from each part of the brain by segmenting it into small voxels (less than 1mm^3)
- Signal returned from each voxel differs depending on the water content of the regions imaged
- Fatty tissues (e.g myelin sheath around white matter) are lower in water than grey matter
o CSF has greatest water content - Generates one high resolution depiction of brains structure and usually takes 7-10 minutes to record
- Describe how functional MRIs work
- Measures the amount of activation in each voxel (less than 2-3mm^3)
- Uses same principal as SMRI but condition of magnet and radio pulse are adjusted
- Oxyhaemoglobin and deoxyhaemoglobin in blood have differing paramagnetic qualities
- FMRI targets a reading which differs according to relative balance at each voxel throughout the brain
- Low resolution images generated every 2 seconds and we can passively monitor the brain or run experimentation manipulation
. Define and explain BOLD signal
- Blood oxygen dependent signal
- In fMRI measured variable is called:
- Neural activity is not measured directly, but BOLD fluctuates during an fMRI scan can tell us that particular regions required more oxygen at certain times so can infer brain function
- Compare SMRI to FMRI
SMRI
- High resolution (1mm voxels)
- Good contrast between tissue types and spatial resolution
- Suitable for evaluating structural abnormalities but one scan can take several minutes
FMRI
- Low resolution (2mm voxels)
- Many images (every 2 sec for 5 min)
- Indirect measure of neural activity
- Low resolution image but can be updated frequently to evaluate activity changes
- Define and explain voxel based morphology
- VBM is a structural analysis technique
- Used to investigate differences in brain anatomy – grey matter density
- Results highlight regions of the brain which show significant differences in density
- Explain how MRI is illustrated in writeups
- Structural and functional MRI results are typically presented on top of a recognisable brain structure
- Illustrated by overlaying on top of a sample structural image which provides spatial context
- In FMRI only coloured blob data actually comes from study in question
- Explain why statistical methods are needed in MRI studies
- Studies give a rich data set – typical resolution gives 6000 voxels per 2 second scan
- 20 min experiment gives 7.2 million data points
- At p<0.05 we can expect 360,000 false positives > risk of type 1 error
- Need to perform many comparisons – good MRI methods compensate for this with statistical corrections
- Give research findings for plasticity in mirror box therapy
- Guo (2016) – showed enhanced bilateral somatomotor activation in patients following MBT
- Michielson (2011) – only deep limbic areas demonstrated changes following MBT
- Give research findings for plasticity in stroke recovery
Rehme and Fink et al (2011) – patients recovery correlated with the ability of contralateral cortex to activate during movement of affected limb
- Ipsilateral activation represents maladaptive plasticity
- Give research findings for plasticity in CBT patients
CBT may impact on brain structure and function
- Siegle and Carter (2006) – depressed patients demonstrate disrupted emotional regulation
o Also show enhanced brain activity (FMRI) in amygdala during emotional stimuli
o Patients with greatest degree of amygdala dysfunction benefited from greatest improvement post CBT
- Give research findings for brain training
Meta-analyses questioned the benefits of brain training
- Likely to be specific to the trained task
- Kable et al (2017) Brain imaging shows no reputable changes in brain function for wider cognitive tasks after training
- Better evidence for brain benefits of physical exercise
- Give some examples of hypothalamic releasing and inhibitory hormones and their functions
- Thyrotropin-releasing hormone = TRH
o stimulates secretion of thyroid-stimulating hormone in anterior pituitary - Gonadotropin-releasing hormone = GnRH
o stimulates secretion of LH and FSH in anterior pituitary - Corticotropin-releasing hormone = CRH (from paraventricular nucleus)
o stimulates secretion of adrenocorticotropic hormone in anterior pituitary - Growth hormone-releasing hormone = GHRH
o stimulates secretion of growth hormone in anterior pituitary - Growth hormone-inhibitory hormone = somatostatin
o Inhibits secretion of growth hormone in anterior pituitary - Prolactin-inhibiting hormone – PIH (dopamine)
o inhibits secretion of prolactin in anterior pituitary
- Give some of the hormone types released by the anterior pituitary
AP contains cells of different types specialised for secretion of different pituitary hormones:
• somatotropes
• corticotropes
• thyrotropes
• gonadotropes
• lactotropes
- Give some examples of hormones and their functions released from the anterior pituitary
- Growth hormone – somatotropin – GH
o stimulates body growth, cell multiplication and Differentiation - Adrenocorticotropic hormone – ACTH
o stimulates secretion of glucocorticoids and androgens in adrenal cortex - Thyroid stimulating hormone – TSH
o stimulates secretion of thyroid hormones - Follicle-stimulating hormone – FSH
o stimulates development of ovarian follicles and spermatogenesis in testis - Luteinizing hormone – LH
o causes ovulation and stimulates the corpus luteum; stimulates secretion of estrogen and progesterone in ovaries; stimulates testosterone in testis - Prolactin – PRL
o stimulates milk secretion and development of mammary glands
- Give the role of glucocorticoids
Hormones that help to cope with stress (trauma, cold, infection, surgery, psychological stress)
• increase glucose level (for muscles)
• supports genesis of new glucose
• mobilises free fatty acids (energy)
• mobilises amino acids (new proteins?)
• decreases immune responses
• increases proteins in liver and plasma (healing of injured tissues?)
• decreases inflammation
• strengthening of catecholamine effects
- What are glucocorticoids regulated by?
ACTH
- Give research findings of dexamethasone
- (Low-dose) dexamethasone suppression test informs about the strength of HPA feedback
- Dexamethasone (a potent glucocorticoid) is applied and the cortisol level is recorded. If HPA feedback works, cortisol level would decrease
- Give 4 ways of evaluated stress using cortisol as a marker
- Resting state cortisol levels, taken from blood or saliva, usually on more than one time point during the day
- Post-stress task increases in cortisol secretion
- Cortisol awakening response – using the natural morning increase in cortisol secretion
- Low-dose dexamethasone suppression test
- Give some types of pain
- Pain can be produced by nociceptors (free nerve endings) responding to heat, cold, chemicals and pressure= nociceptive pain.
- Pain can be caused by a lesion or in jury of a nerve = neuropathic pain.
- Pain can be also caused by dysregulation within central nervous, hormonal or immune system = nociplastic pain.
- Explain the difference between acute and chronic pain and give some chronic pain conditions
- Acute pain: pain lasting hours/days/weeks (e.g toothache, injuries)
- Chronic pain: pain lasting more than 3 months
o Chronic pain syndromes:
Fibromyalgia – widespread pain in soft tissues
IBS – painful sensations in abdomen
• Nociplastic pain
Lower back pain
Headaches – migraine (unilateral, pulsatile pain)
Arthritis – pain in the joints due to wear and tear (osteoarthritis) or autoimmune response (rheumatoid
- Define and explain allostasis
- Allostasis: achieving stability through change
- Active process aimed at achieving balance.
- Examples: turbulence during a flight, focusing on a difficult task, bereavement, finding food in extreme conditions, imprisonment.
- Define allostatic load and overload
- Allostatic load – cumulative effects of allostatic state. It is a sum of responses
sub-serving fulfilment of daily routines plus extra demands. - Allostatic overload – wearing and tearing of allostatic resources if:
- the stress is too strong or prolonged (chronic)
- the coping resources diminish, e.g., due to unrelated disease or ageing
• Leads to a dysregulation of physiological systems including the brain and can lead to a chronic condition such as psychiatric disturbances, chronic fatigue syndrome or chronic pain.
• Dysregulation of the HPA and brain neurotransmitter systems due to allostatic overload is a probable cause of chronic diseases
- Describe the background of and findings of stress induced analgesia
- Based on observation of Col. Henry
o Beecher (1946) on soldiers sustaining major injuries in combat zones of WW2.
o 73% of wounded soldiers did not require any morphine. - “Stress-induced analgesia is a built-in mammalian pain suppression response that occurs during or following exposure to a stressful or fearful stimulus” (Butler and Finn, 2009).
- Physical exercise, acute fear or conditioned fear typically induce stress analgesia.
- SIA– part of fight or flight response, improves chances of survival
- Give the two models of stress-induced analgesia
- Unconditioned SIA – analgesia during concurrent exposure to an unconditioned stressor (e.g., cold, strenuous exercise, presence of predator, infantile isolation)
- Conditioned SIA (Fear-conditioned analgesia)– re-exposure to the context or environment at which the animal had experienced an unconditioned stressor
- Example: A rat exposed to forced swimming in cold water will show analgesia when brought again to the same water tank
- Give animal research findings of SIA
- Rodent animals selectively bred to show high or low pain suppression during stress reveal (see Butler and Finn, 2009):
- High-SIA animals show greater sensitivity to opioids (morphine) and their antagonists (naloxone) than low SIA animals.
- High-SIA animals have abundance of m-opioid receptors in their brains.
- Administration of naloxone blocks the SIA.
- Descending inhibition via the endogenous opioid system of spinal cord transmission of nociceptive impulsive is the main mechanism of SIA.
- Describe the neuronal pathways in SIA
- Glucocorticoid receptors are in abundance in prefrontal cortex, hippocampus, amygdala and hypothalamus =corticolimbic system
- Prefrontal cortex, hypothalamus, amygdala and hippocampus project to periaqueductal grey matter
- PAG sends impulses to rostro-ventromedial medulla (RVM) via endogenous opioids
- RVM activates nucleus coeruleus (noradrenergic), serotoninergic and cannabinoid (CB1) neurons to exert descending inhibition onto nociceptive processing in the spinal cord
- Explain how naloxone can attenuate SIA
Repetitive electrical stimuli to a peripheral nerve at the ankle under the stress showed a progressive increase in thresholds of the defensive twitch response. Naloxone reduced the stress-induced increase in pain thresholds.
- Do corticoids strengthen SIA?
Rats after hypophysectomy do not show SIA when swimming in cold water (Bodnar et al., 1979, in Butler and Finn, 2009).
• Administration of metyrapone (a drug that stimulates secretion of ACTH) caused increased SIA in rats during exposure to hot plate (pain stimulus) after swimming in cold water (stress) (Moussa et al., 1981).
• Systemic administration of dexamethasone which blocks the HPA reduced the strength of SIA in rats (see Butler and Finn, 2009).
- Give some of the neurotransmitter systems involved in SIA
Endogenous opioid peptides and their receptors (mu, kappa, delta)
• Systemic administration of naloxone and other antagonists of endogenous opioids attenuates SIA and FCA
• Administration of morphine strengthens SIA
• The opioid neurons exert their effects via GABA and glutamate
• GABA (gamma amino-butyric acid)
• Glutamate (NMDA receptors)
• Monoamines (noradrenaline, dopamine, serotonin)
• Cannabinoids (CB1 receptors)
- Describe and explain stress-induced hyperalgesia
Enhanced pain experience in the presence of stress
- SIH – when stressors are mild, prolonged, repetitive
- Examples of SIH-type stressors in animals:
- exposure to cold, immobilisation, air stress, holding, anticipation of aversive stimuli
- In humans: anxiety, bereavement, chronic illness, difficult tasks spanning over long periods of time, redundancy, marital problems
- Stressor time scale: days-weeks-months
- SIH likely in presence of a continuously heightened arousal
Describe the transactional model

describe the changes in brain activity during sleep (awake to stage 2)

describe the changes in brain activity during sleep (stage 3 to REM sleep)

Describe the types of brain activity during sleep
Awake: Alpha activity, beta activity
Stage 1 sleep: Theta activity,
Stage 2 sleep: Spindle, K complex
Stage 3: Delta activity
Stage 4: Over 50% delta activity
REM: theta activity, beta activity (most similar to awake EEG)

Describe the endocrinology of menopause

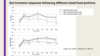
describe the mechanism of starting a meal

Describe the mechanism of ending a meal

Describe the mechanism of CCK and glp-1