Spine Flashcards
Name the #

Chance #: horizontal splitting of the spinal canal, w/anterior wedge compression # + horizontal # through the posterior elements or distraction of the facet joints & spinous processes.
- No retropulsion is often seen.
- Flexion/distraction #s.
- Involved all 3 columns–very unstable.
- All 3 ligaments torn: ant/post spinal ligaments, longitudinal spinal & ligamentum flavum.
- High assocn w/intra-abdo injuries: 65% pancreas & duodenum.
- Most commonly in upper lumbar & thoracolumbar junction.
- Associated w/lap-band seatbelt & no shoulder strap, i.e., back seat passenger.
Dx? 34yo male w/neck pain after a weight-lifting accident.

Clay shoveler’s #: avulsion of a lower cervical/upper thoracic spinous process w/ “ghost sign”.
- “ghost sign” = double spinous process on the AP.
- Usually C7.
- From forceful hyperflexion, like shoveling.
- Can also occur w/direct trauma to the area.

- Name the injury.
- What is its hallmark?

- Hangman #.
- Bilateral C2 pars interarticularis #s.
- Seen most commonly when the chin hits the dashboard in an MVA.
- Can occur through pedicles, but less commonly.
- There is often an associated # at the anterior/inferior corner of C2.
- Cord damage is uncommon as the pars defect widens the canal.
- 3 types, classified by the Effendi classification.
-
Next steps:
- Look for odontoid & C1 #s.
- Get CTA to look at vertebral arteries.
Which type of C1 # (Jefferson) is considered the most unstable?

- Burst # w/disruption of transverse ligament.
- Sum of lateral displacement of the lateral masses of C1 over C2 (>7mm) is a sign of transverse ligament injury (rule of Spence).
- 30% will have a C2 #.
- Cord damage is rare b/c all of the axial loading force is directed into the bones.
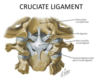
What is the difference b/w the alar & transverse ligaments?
Alar:
- Attaches the dens to the skull.
Transverse:
- Part of the cruciate ligament.
- Attaches the body of the dens to C1.
- If C1 is disrupted (Jefferson #), then if the lateral masses are slipped >7mm then the xverse ligament is likely ruptured.
Which MR sequence can be used to detect acute cord hemorrhage?
T2* (susceptibility weighted images)

What is the most common cause of vertebra plana in kids?
- eosinophilic granuloma
- What is suggestive of screw loosening in pts w/fusion hardware?
- What is an indication of possibly motion across fused spinal levels?

- >2mm lucency around the screw.
- Centrally interrupted trabeculation:
Dx?

Emphysematous OM: intraosseous gas.
- Rare but severe.
- Can be caused by the same bug as Lemierre’s (Fusoacterium necrophorum & Clostridium).
- Most often affects the vertebra, sacrum & long bones.

What is the most common cause of this?

Dx: arachnoiditis: empty thecal sac sign.
- Most commonly spinal surgery: occurs in 10-15% of cases.
- Inflammation of the SA space.
- Can alternatively see central nerve root clumping: some or all of the nerves.
Dx? 39yo male recently recovered from an URTI, presents w/bilateral lower extremity weakness & difficulty breathing.

Guillain-Barre syndrome: smooth, diffuse nerve root thickening & enhancement.
- Aka acute inflammatory demyelinating polyradiculoneuropathy.
- Underlying pathology is autoimmune demyelination.
- Ascending weakness (flaccid paralysis) shortly after a viral illness is highly suggestive.
- Most common bug to cause spinal epidural infection?
- How is it spread?
- Strep pneumonia.
- Hematogenously: hence, IVDUs often get these.
- Most common bug to precipitate Guillain-Barre syndrome?
- What 2 other pts are susceptible?
- What is the most commonly affected cranial nerve?
- Which spinal roots enhance more?
- What is the syndrome called if symptoms last >8wks?
- What does this look like–classic sign?

- Campylobacter.
- SLE & lymphoma.
- CN7, facial.
- Anterior >> posterior, which is very strongly suggestive of GBS.
- CIDP: chronic inflammatory demyelinating polyneuropathy.
- Onion bulb nerve roots: thickened.
- Can also see the same thing in Charcot Marie-Tooth disease.
- Can occur after URTI or GI infections.
- Typically, young adults or kids.
- Ascending paralysis & can affect respiratory muscles.
*

- What best describes the function of the dorsal columns?
- DDx for this case?

- Sensory: fine touch, vibration, proprioception.
- Inverted V sign: Vit B12 deficiency, HIV, HSV, ADEM.
- Dx:?
- What serum abnormality may be seen here?
- Early in the disease, what happens to the SI joint?

- Ank spond: fused syndesmophytes, bilateral SI joint fusion & chronic L3 #.
- CRP.
- Ank spond is a seronegative spondyloarthropathy, so RF is absent.
- Subchondral bone resorption along the iliac side of the SI joint.
Dx?

Vit B12 deficiency: “inverted V-sign”, bilateral, symmetrically increased T2 signal of the dorsal columns w/o enhancement.
- Aka subacute combined degeneration.
- Typically begins in the upper thoracic region & then either ascends or descends.
- DDx: HIV, ADEM.
Name the 1st & 2nd most common intramedullary intradural spinal tumours.

- Schwannoma
- Meningioma:
- The most commonly in the T-spine, followed by C-spine, and rarely in the LS-spine.
- If multiple, think NF-2.
- Calcs are common, like the above.
- Other possibilities: neurofibroma, drop mets.
Dx?

Myxopapillary ependymoma: large, extramedullary, intradural mass at the filum terminal; homogenous enhancement w/low T2 at the margins b/c of hemorrhage; w/scalloping of the vertebral bodies.
- They commonly have tumoral cysts & are long-segment (~4 vertebral bodies).
- They are the most common tumours of the cauda equina region, can also present at the conus.
- Present in younger (35yo) males.
- They can be large & sausage-shaped.

Name the most common intramedullary spinal mass in adults.
Ependymoma.

Name the most common spinal intramedullary tumour in peds?
Astrocytoma
- Favours the upper T-spine.
- Fusiform cord dilation over multiple segments.
- Eccentric.
- T1 dark, T2 bright & enhance.
- May have associated cysts/syrinxes.

Dx of this lesion & specifically if there are cutaneous lesions.

Neurofibroma (nerve sheath tumour): envelops the adjacent nerve root.
NF-1 (NF-2 lacks cutaneous manifestations).
What Ix sign suggests a specific diagnosis?

- Flow void = paraganglioma.
Dx?
- Classic presentation?

Osteoid osteoma: central nidus (<1.5cm) w/surrounding dense sclerosis; T2 hypoenhancing nidus surrounded by T2 hyperintense edema & enhancing reactive zone.
- Night pain relieved w/aspirin or painful scoliosis.
- 75% in the posterior elements.
- If >1.5cm then called osteoblastoma.
- Some pts have scoliosis 2dry to muscle spasm.
- Usually pts <30yo.
- RFA can treat them.
In adults, what are the most common non-CNS solid tumours to present w/leptomeningeal mets?

- Lung & breast ca, but lymphoma can too.
Dx?

Hemangioblastomas (vHL): cyst + nodule; wide cord + considerable cord edema.
- These can sometimes demonstrate flow voids.
- Thoracic level is most common, 2nd most = cervical.
- Panc cysts are common.
- 25-40% of hemangioblastomas occur in pts w/vHL.
- AD disease.
- In vHL, 75% occur in the cerebellum, 25% in spine.

Dx? 30yo female.
- Which vessel wall layer is typically affected?

Takayasu arteritis: thick soft tissue circumferentially around the L ICA & string-like narrowing of the R ICA.
- All 3 layers of vessel wall, typically beginning w/adventitia then working inwards.
- Involves the Ao & its major branches.
- Pulmonary artery involvement may also be seen.
- Most common in younger females.
- Can present w/TIAs & HTN, also fever, wt loss & fatigue.

TvT: astrocytoma vs. ependymoma

Dx?

Aggressive spinal hemangioma: normal-appearing vertebral hemangioma but w/soft tissue component narrowing the spinal canal.
Dx? Male w/genetic disorder.

Dural ectasia/dysplasia in NF-1: enlargement of the CSF spaces w/scalloping of adjacent bone.
- Dx; 45yo male?
- What syndrome can result from this?

Dural AV fistula: innumerable T2 flow voids along the dorsal surface of the cord; the cord is usually swollen & w/high T2 signal.
- Foix-Alajouanine syndrome: cengestive myelopathy 2dry to venous congestion/HTN.
- Classic Hx is a 45yo male w/LE weakness + sensory deficits.
- Will see high T2 signal in the cord.
- Most common in T-spine.
- Fistula b/w the dorsal radiculomedullary arteries & radiculomedullary vein with the dural nerve sleeve.
- Gold standard for Dx is angiography.

Dx? Dizziness & abnormal neck Doppler.

Subclavian steal: occuluded proximal L subclavian a. w/flow in the post-vertebral segment via the patent L vertebral a.
- This results in retrograde flow in the ipsilateral vertebral artery on US.
- Can also occur in the innominate a.
- These pts often have upper extremity claudication as the retrograde flow may not be sufficient for adequate tissue perfusion.

- Which sequence was used to obtain this image?
- What is it showing?

- Phase-contrast sequence CSF flow.
- Lack of flow-related signal in the dorsal SA CSF space at the cervicomedullary junction, compatible w/crowding 2dry to tonsillar ectopia (Chiari I).

Dx, 2 different pts?

Chiari 1: tonsillar ectopia w/syrinx seen in upper cord of 2nd pt.
- Inferior displacement of the tonsils below the foramen magnum >=5mm.
- May be idiopathic or 2dry to posterior fossa or craniovertebral junction abnormalities.
- Caudally-displaced tonsils are typically pointed or peg-like.
- The most common complications result from altered CSF flow dynamics & include syrinx or hydrocephalus.
- Chiari 1.5: a new entity which is Chiari 1 + inferior brainstem descent (typically the inferior margin of the 4th ventricle (obex)).
- Tx: suboccipital craniectomy & often resection of the posterior arch of C1 to restore normal CSF flow.

Dx?

Lipomyelocele: fat located b/w the neural placode ventrally & spinal defect dorsally, but w/overlying intact skin; w/tethered cord & terminal syrinx; expansion of the lumbar spinal canal.
- The neural placode lipoma interface lies w/in the spinal canal.
- This is an intraspinal lipoma in contiguity w/the subcutaneous fat via the defect in the posterior elements.
- If the neural placode projects through the defect into the subcutaneous tissues then this would be a lipomyelomeningocele.
- The lipoma may be intra- or extradural.
- There is typically mild expansion of the spinal canal & distension of the SA space at the level of the defect.
Dx?

Caudal regression syndrome (type 1): sacral agenesis beyond S1, early termination of the conus (at T11-12), which also appears blunted.
- Type 1: high termination of the conus (above L1), which is blunted or wedge-shaped, typically assoc w/sacral anomalies above S1.
- Often w/associated GU or GI malformations, commonly: renal agenesis, hydronephrosis, anal atresia & imperforate anus.
- Also often have vertebral segmentation anomalies.
- Associated w/diabetic embryopathy.
Dx?

Caudal regression syndrome, type 2: low-lying, tethered cord w/less severe sacral agenesis, here, which is coccyx agenesis.
- Low-lying, tethered cord w/less severe sacral agenesis, typically below S2

Dx?

Fatty filum terminale (aka fibrolipoma): high T1 signal w/in the filum at L4-S1, which is suppressed on STIR images; normal conus position.
- Conus terminates at the normal position.
- Refers to fat in an otherwise normal size filum (transverse diameter <2mm).
- Most commonly is incidental & no further Ix required.

Dx?

Terminal ventricle: dilation of the distal central canal in the distal spinal cord.
- Aka ventriculus terminalis or 5th ventricle.
- C-E MRI is instrumental to show lack of enhancement, nodularity or septations in pts w/suspected conus neoplasms.
- Incidental finding, often found in kids; no additional f/u required.
Dx?

Chiari I: small posterior fossa w/inferior displacement of the vermis, cervicomedullary kinking, tectal breaking & flattening of 4th vent.
- Small posterior fossa cannot accommodate the growing brainstem & cerebellum.
- The cerebellum is displaced superiorly w/mass effect on the tectum, causing beaking, as well as inferiorly, flattening the 4th vent.
- Nearly all pts have myelomeningocele.

Dx?

Diastematomyelia.
- 2 types:
- 2 hemicords w/2 dural sheaths.
- 2 hemicords w/a common dural sheath.
- Commonly assoc w/vertebra segmentation anomalies & spinal dysraphism.
- May have progressive scoliosis or cutaneous stigmata, e.g., hairy patch (>50% of cases).