Exam 4 - Reproductive Flashcards
What are the current recommendations regarding self-breast exams?
- USPSTF* recommends against teaching BSE d/t evidence that it doesn’t reduce mortality and may lead to higher rates of benign breast biopsies
- American Cancer Society* recommends against BSE, but states all women should be familiar with how their breasts normally look and feel
What are the current recommendations regarding breast cancer screening - USPSFT?
Mammography
- 50-74 years - biennially
- <50 years - individualize screening based on patient specific factors
- >75 years - insufficient evidence to recommend
Clinical breast exam
- >40 years - insufficient evidence to assess additional benefits and harms of CBE beyond screening mammography
What are the current recommendations regarding breast cancer screening - American Cancer Society?
Mammography
- 40-45 years - optional annual screening
- 45-54 years - annual screening
- >55 years - biennial screening w/ option to continue annual screens
- Continue screening if good health and life expectancy >10 years
Clinical breast examination
- Not recommended d/t lack of evidence showing clear benefit
What are the current recommendations regarding breast cancer screening - American College of Obstetricians and Gynecologists?
Mammography
- >40 years - annually
Clinical Breast Examination
- 20-39 years - every 1-3 years
- >40 years - annually
What are the seven characteristics of a breast nodule that should be described?
- Location - by quadrant or clock, w/ cm from nipple
- Size - in cm
- Shape - round or cystic, disclike, or irregular in contour
- Consistency - soft, firm, or hard
- Delimination - well circumscribed or not
- Tenderness
- Mobility - in relation to skin, pectoral fascia, chest wall
What history, exam findings, and risk factors are consistent with a fibroadenoma?
Usual age: 15-25 years, usually puberty and young adulthood
Shape: round, disclike, or lobular; typically small (1-2 cm)
Consistency: soft
Delimination: well delineated
Mobility: very mobile
Tenderness: nontender
Retraction signs: absent

What history, exam findings and risk factors are consistent with a cyst?
Usual age: 30-50 years, regress after menopause except w/ estrogen therapy
Shape: round
Consistency: soft to firm, usually elastic
Delimination: well delineated
Mobility: mobile
Tenderness: often tender
Retraction signs: absent

What history, exam findings and risk factors are consistent with cancer?
Usual age: 30-90 years, most common >50 years
Shape: irregular or stellate
Consistency: firm or hard
Delimination: not clearly delineated from surrounding tissues
Mobility: may be fixed to skin or underlying tissues
Tenderness: usually nontender
Retraction signs: may be present

What are some visible signs of breast cancer?
Retraction, dimpling, edema, abnormal contours, nipple retraction and deviation, Paget diease of nipple

What could milky nipple discharge indicate?
Milky discharge unrelated to prior pregnancy and lactation is nonpuerperal galactorrhea
Causes: hyperthyroidism, pituitary prolactinoma, dopamine antagonists (psychotropics and phenothiazines)
What could bloody nipple discharge indicate?
Spontaneous unilateral bloody discharge from one or two ducts indicates:
- Intraductal papilloma
- Ductal papilloma in situ
- Paget disease of the breast

What could clear, serous, green or black nipple discharge indicate?
Usually benign
What are considered normal findings of the breasts of newborns?
Breasts of the newborn in both males and females are often enlarged from maternal estrogen effect (may last several months)
May be engorged w/ white liquid (“witch’s milk”) which lasts 1-2 weeks
What is premature thelarche?
Breast development occurs, most often between 6 months and 2 years
Other signs of puberty or hormonal abnormalities not present
What are the current recommendations regarding testicular self-exams?
USPSTF - inadequate evidence for the benefit of screening, either by clinician or self-examination
- Advised against screening for testicular cancer in asymptomatic adolescent or adult males
American Cancer Society - recommends that testicular examination should be part of general physical exam, but no recommendation for self-examinations
- Advises males to seek medical attention for any of the following: painless lump, swelling, enlargement in either testicle, pain or discomfort, feeling of heaviness or sudden fluid collection in scrotum, dull ache in lower abdomen or groin
What symptoms and exam findings are consistent with a testicular torsion?
- Tender painful scrotal swelling
- Retracted upward in scrotum
- Absent cremasteric reflex on affected side
- No associated urinary infection
Most common in neonates and adolescents; surgical emergency

What is the cremasteric reflex and how is it performed?
Examine the child when he is relaxed b/c anxiety stimulates the cremasteric reflex
Have patient sit cross-legged, give him a balloon to inflate, or an object to lift to increase intra-abdominal pressure
Option 1: Warm hands, palpate lower abdomen, work way down towards scrotum along inguinal canal (minimizes retraction of testes into the canal)
Option 2: Scratch medial aspect of thigh (testes on side being scratched will move up)

What is the difference between a direct and indirect inguinal hernia?
Indirect inguinal hernias develop at the internal inguinal ring, where the spermatic cord exits the abdomen
Direct inguinal hernias arise more medially d/t weakness in the floor of the inguinal canal and are associated w/ straining and heavy lifting
What exam findings are consistent with gonococcal urethritis vs. nongonococcal urethritis?
Gonococcal urethritis
- Profuse yellow penile discharge
Nongonococcal urethritis
- Scanty white or clear penile discharge
What are some benefits of circumcision?
AAP and experts recommend circumcision d/t reduced rates of HIV and other infections among circumcises males
What type of anticipatory guidance would the FNP provide to the child of the uncircumcised male?
- When bathing your child, wash the penis. Then dry it thoroughly.
- Never forcibly pull back (retract) the foreskin when washing your infant or young child
- When the foreskin is able to retract, gently pull it back and bathe the area. Dry the penis thoroughly.
- Return the foreskin to its natural position by pulling it back over the penis. This is important because if the foreskin is left retracted, it could put pressure on the penis. This can cause pain and swelling and may require medical attention.
What are hypospadias?
Congenital ventral displacement of urethral meatus to the inferior surface of penis
Meatus may be subcoronal, midshaft, or at junction of the penis and scrotum (penoscrotal)

What exam findings are consistent with a hydrocele?
Swelling containing serous fluid lights up with a red glow (transilluminates)
Nontender, fluid-filled mass within tunica vaginalis
Examining fingers can palpate above the mass within the scrotum

How would the FNP classify Tanner Stages (Sexual Maturity Rating) in males?

What is the general order of pubertal changes in the male?
- First reliable sign of puberty, between ages 9-13.5 years, is increase in size of testes
- Pubic hair appears along w/ progressive enlargement of penis

Can you identify the external female anatomy?
- Mons pubis
- Prepuce
- Clitoris
- Urethral meatus
- Opening of paraurethral (Skene) gland
- Vestibule
- Introitus
- Perineum
- Labia majora/minora
- Hymen
- Vagina
- Opening of Barthlin gland
- Anus

What are the differences in symptoms, exam findings and wet mounts finding for: trichomonal vaginitis, candidal vaginitis, and bacterial vaginosis?
Discharge
- Yellowish green/gray, possibly frothy
- Profuse and pooled in vaginal fornix
- Malodorous
Symptoms
- Pruritus (not as severe as candida infection)
- Pain w/ urination
- Dyspareunia
Vulva and vaginal mucosa
- Vestibule and labia minora may be erythematous
- Vaginal mucosa diffusely reddened w/ small red granular spots or petechiae in posterior fornix
Lab evaluation
- Scan saline wet mount for trichomonads

What are the differences in symptoms, exam findings and wet mounts finding for: trichomonal vaginitis, candidal vaginitis, and bacterial vaginosis?
Discharge
- White and curdy; may be thin but typically thick
- Not malodorous
- Not as profuse as in trichomonal infection
Symptoms
- Pruritus, vaginal soreness
- Pain w/ urination
- Dyspareunia
Vulva and vaginal mucosa
- Vulva and surrounding skin often inflammed and swollen
- Vaginal mucosa reddened w/ white tenacious patches of discharge
- Mucosa may bleed when patches are scraped off
Lab evaluation
- Scan KOH preparation for branching of hyphae of candida

What are the differences in symptoms, exam findings and wet mounts finding for: trichomonal vaginitis, candidal vaginitis, and bacterial vaginosis?
Discharge
- Gray or white, thin, homogenous, malodorous
- Coats vaginal wall
- Usually not profuse
Symptoms
- Unpleasant fishy or musty genital odor
- Reported to occur after intercourse
Vulva and vaginal mucosa
- Usually appear normal
Lab evaluation
- Scan saline wet mount for clue cells (epithelial cells w/ stippled borders)
- Sniff for fishy odor after applying KOH (“whiff test”)
- Test vaginal secretions for pH >4.5

What are some tips for a successful pelvic exam?

What are some normal configurations of the hymen in the prepubertal child?
- Two openings
- Crescent shaped hymen
- Annular hymen
- Redundant labial tissue suggesting estrogen effect (possibility of imperforate hymen)
- Annular hymen and hormonal influence of puberty

How would the FNP classify Tanner Stages (Sexual Maturity Rating) in females?

What is the general order of pubertal changes in the female?
Physical changes in girl’s breasts are one of the first signs of puberty
Breasts progress through five stages (Tanner stages)
- Breast buds in preadolescent stage enlarge, changing contour of the breasts and areola
- Aerola darkens in color
- Development of pubic hair and other secondary sexual characteristics

What are some physical signs of sexual abuse in the pediatric patient - strong indications?
- Lacerations, ecchymoses, newly healed scars of the hymen or the posterior fourchette
- No hymenal tissue from 3 o’clock to 9 o’clock
- Healed hymenal transections especially between 3 o’clock to 9 o’clock (complete cleft)
- Perianal lacerations extending to external sphincter

What are the current recommendations for prostate cancer screening?
USPSTF - recommends against screening for asymptomatic men regardless of age, race, or family history
American Cancer Society & AUA - encourage screening average risk patients beginning at ages 50-55 years
Providers encouraged to support shared decision making
- If patient agrees, PSA testing recommended every 1-2 years; DRE optional
- Stop offering screening when patients reach 70 years or when life expectancy drops below 10 years
Providers can consider offering screening beginning at ages 40-45 years to men at high risk for cancer (e.g. African Americans, family history of prostate cancer)

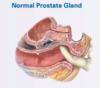
What history and exam findings are consistent with a normal prostate gland?
- Normal prostate is rounded, heart shaped, approximately 2.5 cm long
- Median sulcus can be palpated between two lateral lobes
- Only posterior surface of prostate palpable
- Anterior and central lesions, including those that obstruct the urethra, are not detectable by physical exam
What history and exam findings are consistent with prostatitis?
Acute bacterial prostatitis (pictured)
- Presents w/ fever and urinary tract symptoms (frequency, urgency, dysuria, incomplete voiding, low back pain)
- Gland feels tender, swollen, “boggy”, warm
Chronic bacterial prostatitis
- Associated w/ recurrent UTI
- Men may be asymptomatic or have symptoms of dysuria or mild pelvic pain
- Gland feels normal w/o tenderness or swelling
- Cultures may show infection w/ e. coli

What history and exam findings are consistent with BPH?
Nonmalignant enlargement of prostate that increases w/ age (>50 years)
Symptoms arise from both smooth muscle contraction in prostate, bladder neck, and compression of urethra
- Irritative (urgency, frequency, nocturia)
- Obstructive (decreased stream, incomplete emptying, straining)
- Gland may be normal in size or feel symmetrically enlarged, smooth, firm
- May have obliteration of medial sulcus
- Notable protrusion into the rectal lumen

What history and exam findings are consistent with prostate cancer?
Suggested by an area of distinct hardness (nodule) in the gland
- Nodule may extend beyond confines of the gland
- Obscured median sulcus

What history and exam findings would be consistent with internal hemorrhoids?
Enlargements of the normal vascular cushions located above the pectinate line, usually not palpable
- Bright-red bleeding (especially during defecation)
- Prolapse through anal canal
- May appear reddish, moist, protruding masses

What history and exam findings would be consistent with external hemorrhoids
Dilated hemorrhoidal veins that originate below the pectinate line that are covered w/ skin
- Seldom produce symptoms unless thrombosis occurs
- Thrombosis causes acute local pain that increases w/ defecation and sitting
- Tender, swollen, bluish, ovoid mass is visible at anal margin

What history and exam findings would be consistent with a prolapsed rectum?
On straining for a bowel movement, the rectal mucosa and musclar wall may prolapse through the anus
- Looks like a doughnut or rosette of red tissue
- Prolapse involving only mucosa is small and shows radiating folds (pictured)
- When entire bowel wall is involved, prolapse is larger and covered by concentrically circular folds
