Acid-Base Physiology Flashcards
(73 cards)
Hyperventilation
increased breathing beyond what is required, given the metabolic production of carbon dioxide, to maintain a normal PaCO2
Normal range of PaCO2
36-44 mm Hg
Hypoventilation
Decreased breathing below that which is required for a given level of carbon dioxide production to maintain a normal PaCO2
Hyperpnea
Increased ventilation with a normal PaCO2 (for example, during mild to moderate exercise), i.e., the increase in ventilation is commensurate with the increase in carbon dioxide production.
Tachypnea
Rapid breathing, i.e., a respiratory rate that is above normal. Although total ventilation tends to be elevated in patients who are tachypneic, alveolar ventilation may be normal or greater/lower than normal depending on the tidal volume and the amount of dead space being ventilated
Carbon dioxide elimination is dependent upon ___ ventilation
Carbon dioxide elimination is dependent upon alveolar ventilation
Not necessarily total or minute ventilation
Total ventilation [VE]
VE = VA + VD
a = alveolar
d = dead space
Tractus solitarius
Group of neurons in the medulla whose firing increases with inspiration.
Nucleus retroambigualis
Group of neurons in the medulla whose firing increases with expiration.
Two ‘phases’ of exhalation
- expiratory neurons fire to “brake” the inpiration
- inspiratory activity is completely absent
Electrical activity in inspiratory motor neurons during unstressed breath cycle

Hering-Breuer Reflex
An inspiratory-inhibitory reflex stimulated by pulmonary stretch receptors in the lung during inspiration. Activity is maintained with a sustained stretch
aka slowly adapting stretch receptors
Irritant receptors
Stimulated by mechanical or chemical irritation in the airways. These receptors may be partly responsible for the hyperventilation seen with acute asthma
aka rapidly adapting stretch receptors
Pulmonary vascular receptors
These receptors are part of a group of non-myelinated fibers called C-fibers
Stimulation of receptors in pulmonary capillaries or the interstitium of the lung (juxtapulmonary-capillary or “J” receptors) lead to increased ventilation. These receptors may be responsible for the hyperpnea associated with pulmonary embolism and congestive heart failure as well as interstitial lung disease
Chest wall receptors
Muscle spindles as well as receptors in joints and tendons may help adjust ventilation under conditions of mechanical loading, e.g., patients with airway obstruction. They may also play a role in the hyperpnea of exercise.
Peripheral chemoreceptors
located in the aortic arch and at the bifurcation of the internal and external carotid arteries (receptors in the aortic arch have relatively minor, if any, role in control of breathing in humans); provide input about the PaO2, PaCO2, and pH.
Central chemoreceptors
Located below the ventral surface of the medulla; detect changes in the PCO2/pH of brainstem interstitial fluid
Ventilatory responses to hypoxemia and hypercapnia are measured in ___ experiments.
Ventilatory responses to hypoxemia and hypercapnia are measured in rebreathing experiments.
Hypoxic Ventilatory Response
Hypoxemia results in minimal stimulation of ventilation until the PaO2 decreased to less than 60 mmHg. Stimulation comes from peripheral chemoreceptors, which appear to respond to PaO2 rather than the overall content of arterial blood.
Ventilatory response to hypoxemia
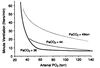
Hypercapnic Ventilatory Response
There is a linear relationship between alveolar ventilation and PaCO2 levels, over a physiologic range.
An increase in PaCO2 results in a much more pronounced increase in ventilation as compared to hypoxemia. Hypercapnia stimulates both peripheral and central chemoreceptors, resulting in an increased drive to breathe.
Hydrogen Ion chemoreceptors
Hydrogen ions cross the blood brain barrier too slowly to have an impact initially on the central chemoreceptors. They do stimulate the peripheral chemoreceptors resulting in an increase in ventilation.
Carbon dioxide diffuses out of CSF as the PaCO2 drops in the systemic circulation with increased ventilation. This lowers CSF carbon dioxide and reduces stimulation of central chemoreceptors. Over time (days), the CSF bicarbonate concentration normalizes.
3 Phases of Ventillation Increase during Exercise
- Neurological Phase - immediate phase
- Metabolic Phase - slowly increasing ventilation during mid-phase of exercise; associated with increasing oxygen consumption
- Compensatory Phase - more pronounced increase in ventilation after anaerobic threshold has been exceeded and metabolic acidosis ensues (the increase in ventilation helps to mitigate the acidosis); more intense exercise.
Neurological Phase of exercise response
Occurs almost instantaneously, far too quickly to be explained by changes in metabolism or blood gases. Felt to be due to “neural mechanisms”- possibly connections from motor cortex to respiratory centers, from skeletal muscle to respiratory centers - or a conditioned reflex or learned response.




