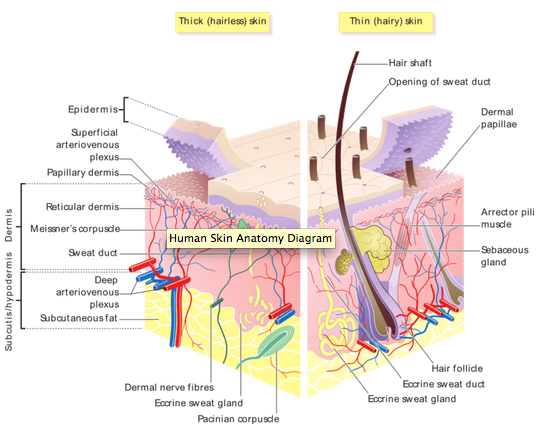
Describe skin anatomy
Describe the different kinds of UV light and their clinical significance:
- wrinkles?
- penetration?
- Vit D synthesis?
- tans?
- burns?
UVC (<290 nm):
UVB (290-320): penetrates less, dierectly damages DNA, responsible for most of Vit D synthesis, the skin tanner
UVA (320-400): Penetrates most deeply, most damage is from damage to photosensitive things in cell which then directly damage DNA, the skin burner and wrinkler and sagger
What is the standard model of carcinogenesis in skin cancer? What kind of exposure are SSC and BCC linked with?
- Tumour induction (inital DNA damage- even low does of UVB can do this)
- Tumour promotion (usually multiple required)
SSC: long term UV exposure
BSC: intermittent bouts
What is melanin? Where is it produced? What are the different types? What are it’s functions?
Pigment that protects the skin from UV damage. Produced in melanosomes (tyrosinase) in melanocytes found in the stratum basale and transferred to adjacent keratinocytes (1 melanocyte can supplie 36 keratinocytes)
Eumelanin: most protective
Pheomelanin: less proctective, found in redheads
Functions:
- protect from UV light
- scavenge free radicals
- neural development
What is the typical presentation of BCC? Do they metastasize?
Site: sun exposed areas, e.g. face
Appearance: erthematous nodule with telangiectasia, may have ulcer with rolled edge, pearly or translucent. Can be pigmented. Can also be superficial (as opposed to nodular)
Arises from keratinocytes in the stratum basale, are locally invasive, but don’t usually metastasize
What are the clinical features of SCC? Metastatic potential?
Derived from suprabasal keratinocytes
Where: Usually on areas of maximum sun exposure
Cause: prolonged UV exposure
Appearance: hard pink or white nodule, scaling
Has metastatic potential
What are the precursors to squamous cell carcinoma?
Actinic keratosis
SSC in-situ (Bowen’s disease
What are treatment options for actinic keratosis? Why does it need to be treated?
- cryotherapy
- topical 5-FU (pyrimidine suicide inhibitor)
~10% evolve into SCC if left untreated
What are treatment options for SCC and BCC and melanoma?
SCC
- surgical excision
- radiation
BCC
- electrodissecation and curettage
- simple excision
- micrographic surgery (Mohs)
- radiation therapy
Melanoma:
- surgical, maybe with lymph node dissection
- can try chemo if systemic, but poor response
What is Mohs surgery?
They remove the lesion with as narrow borders as possible, then look at the boders under the microscope to see if they are clear. If they aren’t, they remove a little more. all happens in the operating room.
What is a nevus, where does it come from and what is the typical evolution? What is an atypical nevus?
A nevus is a from sun-damaged melanocytes. A nevus is a nest of abnormally dividing melanocytes.
1) Junctional nevus (at the dermal-epidermal junction)
2) Compound nevus (in both)
3) Dermal nevus (entirely within dermis
An atypical nevus cannot evolve in the typical sequence to a dermal nevus so it has irregular edge and color and spreads sideways instead of down into the dermis. It is at high risk to progress to melanoma
What is the most significant risk factor for developing melanoma? What’s the most important prognostic factor of melanoma?
>100 nevi (risk 1:10 vs. 1:90)
tumous thickness- correlates with survival and metastasis potential
What are the ABCDE’s of melanoma?
Asymmetry
Border
Color
Diameter
Evolution
What are the types of melanoma?
Superficial spreading melanoma: when nevi become melanoma, it’s usually this
Nodular: develops without an obvious precursor lesion
Lentigo maligna melanoma: starts as brown patch, cells are along the dermal-epidermal junction, eventually nodule appears
What is SPF?
Sun-protective factor: the amount of time required to burn with the sunscreen on divided by the amount of time required to burn without the sunscreen.
Most of us only apply 1/3 of what is needed to acheive the lable spf….
What is the embryologic orgin of the dermis and epidermis?
epidermis: ectoderm (melanocytes are neural crest origin)
dermis: mesoderm
Describe the layers of the epidermis
- Stratum basale :single layer keratinocytes, melanocytes (have smaller darker nucleus and halo). attached to BM by hemidesmosomes
- Stratum spinosum: polygonal keratinocytes attached via desmosomes
- Stratum granulosum: flattened cells with keratohyaline granules
- Stratum corneum: coreneocytes- cells have lost nucleus and organelles
How to tell keratinocytes and melanocytes apart on LM?
Keratinocytes: tonofilaments –>desmosomes
Melanocytes: melansomes (dark-skinned people have more melanosomes, not more melanocytes)..have smaller nucleus than basal keratinocytes and a halo (they are rigidly bound to neighboring cells like keratinocytes are)
What are langerhans and Merkel cells (where are these most abundant)?
Langerhans: tissue dendritic cells. found in stratum spinosum. hard to see on LM. has Birbeck granules
Merkel: cells associated with free nerve endings- touch receptors. found in stratum basale and at the base of follicles. most abundant in acral skin
What are the 3 mesenchymal layers of the skin?
- Papillary dermis: loose elastin and collagen
- Reticular dermis: thick collagen and ellastin
- Subcutis: lots of fat
Describe blood and nerve supply to the skin
Superficial plexus: btw papillary and reticular
Deep plexus: btw reticular and subcutis
Glomus bodies are specialized arteriovenous shunts in the deep dermis. highest # in acral skin
Nerves mostly found in dermis
- encapsulated: touch
- free: temperature, pain
- specialized: Meissner (in papillary dermis), Pacinian (in deep dermis/subcu)
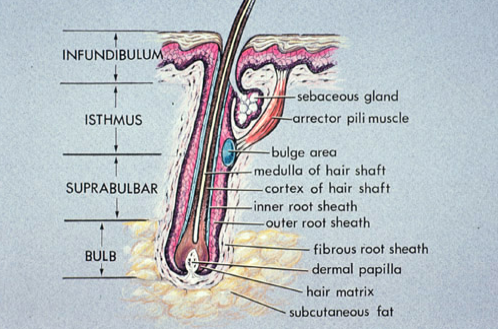
Structure of a pilosebaceous unit
Differentiate apocrine, holocrine and merocrine (eccrine) secretion
Apo: a chunk of cell is secreted (an “apex”)
Holo: the whole cell is secreted, as in sebaceous glands
Merocrine: vesicles are released, as in sweat glands
Differentiate apocrine and eccrine (merocrine) sweat glands
Apocrine: only found in groin, axilla, external ear (ceruminous glands), nipple, eyelid (Moll’s gland). empty into hair follicles. smelly sweat
Eccrine: release contents directly to skin (coil–>straight duct–> acrosyringium). straight portion is responsible for reabsorbing salt. coiled portion essentially releases an ultrafiltrate


