Anatomy, MCP and Histology Deck Flashcards
(221 cards)
What components of the cell is labeled by hematoxylin stain?
-heterochromatin, RER, and sulfated GAGs
What components of a cell are labeled by Eosin stain?
cytoplasm, cytoplasmic filaments, and collagen fibers and basment membrane
What type of epithelium is best designed to protect against abrasion?
Stratified squamous epithelium
What two functions of simple squamous epithelium?
active transport via pinocytosis and secretion of biologically active molecules
Define stereocilia
microvilli of the male reproductive tract
Define striated border
microvilli of Intestinal Epithelial cells
Define brush border
is the microvilli of renal proximal tubule
What is hyperplasia mean?
means an increase in cell number
what is hypertrophy?
increase in size
what is dysplasia?
change in organization
what is metaplasia?
transformation to another cell type
Compare cilia vs. microvilli
cilia:
-microtubules in a 9+2 arrangement covered by cell membranes
Microvilli:
-finger like extensions on the apical surface of epithelia cells
Name 2 tissues that have basement membrane
simple cuboidal and simple squamous
simple cuboidal functions
corvering and secretion
simple columnar functions
secretion, absorption, lubrication, and protection
strafitied squamous functions
protection (“wear and tear”), and prevention of water loss
ie. anal canal, mouth, vaginal canal and skin
Stratified cuboidal functions
protection and secretion
what functions of transitional epithelium?
Protection and distensibilty
Stratified Columnar functions
Protection
Dense Regular Loose CT what is it
- more
- loose connective tissue which has more fibers than cells
- forms parallel bundles or sheets
- found in tendons, ligaments, and cornea
Dense irregular CT
- loose CT that there are more fibers than cells
- fibers are interwoven
- found in organ capsules, periosteum, and reticular layer of dermis
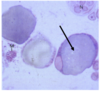
What cell is virtually stained with trypan blue
Macrophages
What cell is identified in the blue? What is the stain used

Macrophages
Trypan blue
The cell that is the most common CT cell
Fibroblasts