Anterior Abdominal Wall, Inguinal Canal, and Scrotum (Part 1: Anterior Abdominal Wall) Flashcards
(76 cards)
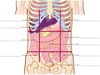
2 parts of abdominopelvic cavity
1) abdominal cavity proper (orange)
2) pelvic cavity (false pelvis) (green)

where does the abdominal cavity end and the pelvic cavity begin?
At the pelvis inlet (pelvic aperture)

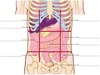
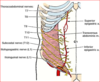
Superior border of the abdominal cavity:
Superior border: diaphragm and costal margin (ribs 7-10) + 11th and 12th ribs

Inferior border of the abdominal cavity
Inferior border: Pelvic inlet (pelvic brim)

Anterior and lateral border of abdominal cavity
Anterior and lateral border: skin, fascia, and muscles (musculo-aponeurotic)

Posterior border of the abdominal cavity:
Posterior border: lumbar vertebral column, back muscles, diaphragm that overlies the thoracic vertebrae and lower ribs

A =


B =


C =


D =


E =


F =


G =


A =


B =


C =


D =


E =


F =


G =


H =


I =


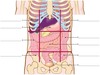
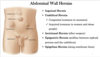
tendinous intersections
tendinous intersections run horizontally across each rectus abdominis muscle

anterior superior illiac spine (ASIS)
a sharp notch anterior to the iliac crest.