Chapter 20: The Kidney - Congenital, Cystic Dz, Urinary Obstr. and Neoplasms Flashcards
(94 cards)
What occurs to the solitary kidney as a result of unilateral agenesis?
Some pts eventually develop what later in life?
- Solitary kidney enlarges = compensatory hypertrophy, therefore increased risk for HTN
- Some pts eventually develop progressive glomerular sclerosis —> CKD
True renal hypoplasia is most often observed in?
Bilateral or unilateral?
May contribute to an increased lifetime risk for?
- Low birth weight infants
- May be bilateral but is more often unilateral
- Increased risk for CKD
Where is the most common location of Ectopic Kidneys?
May lead to what issues?
- Just above the pelvic brim or within the pelvis
- Ureteral abnormalities may cause obstruction/infection
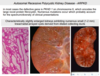
What are the 3 major pathologic features of ADPKD?
Unilateral or bilateral?
- Large, mutlicystic kidneys, bilaterally
- Liver cysts
- Berry aneurysms
Mutation in which gene and on which chromosome account for 85% of ADPKD cases?
PKD1 on chromosome 16
Mutation in which gene and on which chromosome account for 15% of ADPKD cases?
PKD2 on chromosome 4
How does the severity of disease and progression to complications differ between ADPKD pts with a PKD1 vs. PKD2 mutation?
- PKD1 = more severe, increased risk of earlier onset renal failure (95% by 70 yo)
- PKD2 = somewhat better prognosis; less risk of renal failure, at least earlier on.

What are the cysts seen in ADPKD filled with, describe its morphology
Clear serous fluid or turbid red-brown, hemorrhagic fluid
What is the typical clinical course of ADPKD and how does it typically present?
- Generally asymptomatic w/ insidious onset in 4th-6th decade w/ renal insufficiency (HTN, azotemia)
- Some exhibit abd. pain due to cyst enlargement and hemorrhage, thus hematuria may be manifestation
There is a more aggressive (earlier onset, more severe) clinical course in which patients w/ ADPKD?
- Blacks (particularly those w/ sickle cell trait)
- M>F
- Those w/ concomitant HTN
What are the clinically significant extra-renal manifestations of ADPKD?
- Hepatic cysts; less common in spleen, pancreas, and lung
- Berry aneurysms –> subarachnoid hemorrhage
- Mitral valve prolapse
- Many have diverticular dz of colon

How is diagnosis of ADPKD made?
Radiologic imaging
How do the majority of pts w/ ADPKD ultimately end up dying?
Coronary or hypertensive heart disease
Most cases of ARPKD are due to mutation in which gene and on what chromosome?
- PKHD1 on chromosome 6
- Encodes fibrocystin
What are the 2 most common clinical subtypes of ARPKD?
Type of hepatic fibrosis in each?
- Perinatal (most common) –> minimal hepatic fibrosis
- Neonatal –> mild hepatic fibrosis
What is the gross morphology of the surface of the kidneys in ARPKD?
What does a cut section of the kidney show?
- Enlarged w/ SMOOTH surface (contast to cystic surface of ADPKD)
- Cut section shows numerous small cysts linearly arrayed in cortex ans medulla w/ spongelike appearance

Where are the cysts seen in ARPKD derived from?
Dilated collecting ducts
What is the typical clinical course of ARPKD?
- Perinatal form = most common; survival only a few hours; death due to pulmonary hypoplasia
- If survive infancy develop congenital hepatic fibrosis —> portal HTN and splenomegaly
In almost all cases of ARPKD the liver contains what?
Cysts associated w/ portal fibrosis and proliferation of bile ducts
What are the 3 major subtypes of medullary cystic disease?
- Medullary sponge kidney
- Nephronophthisis
- Adult-onset medullary cystic disease
What is seen in Medullary Sponge Kidney?
Affected population?
Renal function?
- Mutliple cystic dilations of the collecting ducts and medulla
- Occurs in adults and is usally discovered radiographically
- Renal function is usually normal
What are the disorders characterized as ciliopathies or abnormalities of the cilium-centrosome complex?
- Polycystic kidney diseases (both AD and AR)
- Medullary Cystic Kidney
- Nephronophtisis
In Nephronophthisis-Medullary Cystic Disease where are the cysts localized?
Gross morphology of the kidneys and on microscopy of the cortex?
- Localized to corticomedullary junction and medulla
- Kidneys are small w/ contracted granular surfaces
- Cortex has diffuse atrophy and thickening of tubular BM w/ interstitial fibrosis

What are the 3 clinically recognized variants of the Nephronopthisis-Disease complex?
Which is most common?
- Sporadic, non-familial
- Familial juvenile nephronophthisis (most common)
- Renal-retinal dysplasia



















