CLINICAL DERM Flashcards
(331 cards)
What is the most likely diagnosis?
1 Dermatofibromasarcoma protuberans
2 Dermatofibroma
3 Lobomycosis
4 Blastomycosis
5 Keloid

Keloid
Keloids are dense overgrowths of fibrous tissue that generally form a response to tissue injury. Lobomycosis and dermatofibromasarcoma protuberans may mimic keloids
You suspect that a patient has acquired angioedema. Levels of which of the following would you expect to be low?
1 C1q, C3
2 C1q, bradykinin
3 C4, C1q
4 bradykinin, C3
5 C4, C3

C4, C1q
Initial screening test in angioedema for both inherited and acquired should include C4, which is low. C3 is normal in angioedema. C1q is low in acquired angioedema but normal in the hereditary type. Bradykinin is elevated in both inherited and acquired angioedema.

Cigarette smoking has been shown to:
1 Increase the incidence of BCC
2 Not affect the survival of surgical repairs
3 Demonstrate less solar elastosis than photoaged skin
4 Have no correlation with facial wrinkling
5 Increase cutaneous vasoconstriction
Increase cutaneous vasoconstriction
Cigarette smoking accelerated photoaging. Solar elastosis in patients with significant smoking history is present not only in the papillary dermis, but also the reticular dermis. It has also been shown to increase the incidence of skin cancer, decrease the survival of surgical grafts, increase the severity of wrinkling.
What is the diagnosis of this lesion on the penile shaft?
1 Sclerosing lymphangitis
2 Loaloa
3 Varicose vein
4 Syphilis
5 Lymphogranuloma venereum

Sclerosing lymphangitis
Sclerosing lymphangitis is a self-limited, cord-like structure on the penile shaft, which typically occurs 24-48 hours after vigorous sexual intercourse.
The differential diagnosis for the attached image should include all of the followings except
1 Candidiasis
2 Lichen planus
3 Contact dermatitis
4 Inverse psoriasis
5 Erythrasma

Erythrasma
The image shown is inverse type of psoriasis. Although psoriatic lesions are classically distributed on the extensor surfaces (the elbows, knees, and lumbosacral regions), lesions may also be found in a flexural distribution with involvement of the axillae, groin, perineum, central chest, and umbilical region. Differential diagnosis include all other choices in question. Although erythrasma might be included in differentials in case of groin involvement only, it is unlikly for eryhrasma to presnt on penis with well demarctaed erythamtos plaques. Erythrasma is a superficial bacterial infection of the skin caused by C. minutissimum. It is characterized by asymptomatic, well-demarcated, reddish brown, slightly scaly patches in the groin, axillae, gluteal crease, or inframammary regions, and less often the interdigital spaces of the feet. Erythrasma is frequently confused with a dermatophyte infection, it can be differentiated from tinea infection by the characteristic coral red fluorescence seen when viewed under Wood’s lamp illumination (due to the production of porphyrins by the corynebacteria.
The protein component of nodular amyloidosis is:
1 SAA protein
2 AL protein
3 Keratin
4 Collagen
5 Bp180

AL protein
Nodular amyloidosis presents as single or multiple nodules, often on the extremities. The primary protein component is of the AL type.
AMYLOID = AMMO GUN

What is the most common presentation of psoriatic arthritis?
1 Asymmetric oligo- or polyarthritis
2 Symmetric polyarthritis
3 Spondylitis (axial)
4 Distal interphalangeal joint (DIP) disease
5 Arthritis mutilans

Asymmetric oligo- or polyarthritis
Psoriatic arthritis affects 20-40% of patients with psoriasis. Most (~80%) of psoriatic arthritis patients are rheumatoid factor negative. All of the answer choices represent possible presentations of psoriatic arthritis, but asymmetric oligo- or polyarthritis is the most common presentation.
Which special stain is utilized to confirm the diagnosis of Langerhans cell histiocytosis?
1 H&E sufficient for diagnosis
2 S100
3 CD20
4 CD1a
5 Chloroacetate esterase
CD1a
Langerhan cell histiocytosis includes the diseases Letterer-Siwe, Hand-Schuller-Christian, Eosinophilic Granuloma, and Hashimoto-Pritzker. Cells stain positively with CD1a, S100, and peanut agglutinin. Cells may also be indentified by the presence of Birbeck granules.

What surgical dressing would you use if you wished to debride a wound, reduce pain, and provide a cooling effect?
1 Alginates
2 Foams
3 Hydrocolloid
4 Hydrogel
5 Films
Hydrogel
Hydrogels are 70-90% water, decrease pain, provide a cooling effect, and are useful for dry and necrotic wounds. Foams are suitable for use on light-to-medium exuding wounds. Hydrocolloids ensure the moist wound environment, promote the formation of granulation tissue, and provide pain relief by covering nerve endings with both gel and exudate. Large quantities of alginates are used each year to treat exudating wounds, such as leg ulcers, pressure sores, and infected surgical wounds.

What is the recommended allowance of daily vitamin D intake for a 35-year-old female?
1 200 IU
2 400 IU
3 600 IU
4 800 IU
5 1000 IU
600 IU
Recommended dietary allowance of vitamin D as established by the Institute of Medicine in 2010 is 400 international units for infants 0 to 12 months, 600 IU for ages 1 to 70 years, and 800 IU for ages 71 and above. Additionally, recommended allowance for pregnant/lactating women is 600 IU.
A 35 year-old otherwise healthy man presents with moderate-to-severe plaque psoriasis, improved on cyclosporine. The patient weighs 70 kilograms and is taking a dose of 300 mg/day. His baseline creatinine was 0.8; on follow-up testing it is 1.1. All other exam and laboratory parameters are within normal limits. The patient is pleased with his treatment and asks to continue it. Which of the following is correct?
1 The patient has exceeded the recommeded dosage of cyclosporine
2 You offer a decrease of the cyclosporine dose to 225 mg/day and close follow-up
3 The change in creatinine is not significant, no change is needed
4 Cyclosporine rarely has renal toxicity in young, healthy individuals; thus you must work-up other causes of the increased creatinine
5 The cyclosporine should be stopped immediately; the patient must avoid cyclosporine in the future
You offer a decrease of the cyclosporine dose to 225 mg/day and close follow-up
Cyclosporine is highly effective in most patients with severe chronic plaque-type psoriasis. Doses start at 2.5 to 4mg/kg/day and can go as high as 5.5mg/kg/day. Renal impairment may occur and is often reversible. If the creatinine increases 30% or greater from baseline the dose should be reduced by 25% and the patient followed closely.

A potentially dangerous side effect of spironolactone is:
1 Hypokalemia
2 Hyperkalemia
3 Hypercalcemia
4 Hyponatremia
5 Hypernatremia
Hyperkalemia
Spironolactone is a potassium-sparing aldactone antagonist. Renal failure predisposes patients to potentially dangerous hyperkalemia.

In the absence of the C1 esterase inhibitor, which of the following proteins mediates angioedema most directly:
1 Kallikrein
2 C1
3 Plasmin
4 C3 convertase
5 C2 kinin

C2 kinin
In C1 esterase inhibitor deficiency activated C1 and plasmin generate activated C2 kinin, which mediates angioedema.

Which of the following is true regarding this entity?
1 The subcutaneous variant is most common in children
2 75% of localized lesions are still present 2 years after diagnosis
3 Localized lesions often ulcerate and heal with scarring
4 The perforating variant classically involves the lower extremities
5 Diabetes is present in the majority of patients with the generalized variant

The subcutaneous variant is most common in children
Granuloma annulare is the entity pictured. Subtypes include localized GA, generalized GA, macular GA, subcutaneous GA, and perforating GA. The subcutaneous variant is most common in children; there is often a history of trauma to the area. Localized lesions never ulcerate and heal without scarring; 75% of localized lesions clear within 2 years. The perforating variant classically involves the dorsa of the hands. Diabetes is present in 20% of patients with the generalized variant.
Natural infection with which of the following infectious agents has been shown to mitigate atopic dermatitis?
1 Measles
2 S. aureus
3 Varicella
4 Rubella
5 Coxsackie virus
Measles
Natural measles infection has been shown to ameliorate atopic dermatitis.

A teenager comes into your office requesting laser hair removal of her significant facial hair. Before you agree to treat her, you order which of the following laboratory analyses?
1 FSH and LH
2 Glucose and hemoglobin A1C
3 Ferritin and TIBC
4 Testosterone and DHEA-S
5 TSH and T3
Testosterone and DHEA-S
Hisrutism describes excessive terminal hair growth in areas on women that are normally found only in post-pubescent males (such as beard, chest, inner thigh). Hypertrichosis refers to excessive hair density or length. Hirsutism is under the influence of androgen stimulation. Testosterone and DHEA-S can be used to detect excessive adrenal or ovarian androgen production. Other clinical manifestations of androgen excess in women are acne and virilization.
A 2 year-old boy with crusted skin papules is found to have osteolytic defects and diabetes insipidus. These features are seen in:
1 Osteogenesis imperfecta
2 Conradi-Hunnerman disease
3 Metastatic small cell lung carcinoma
4 Hand-Schuller-Christian disease
5 Epidermal nevus syndrome

Hand-Schuller-Christian disease
Hand-Schuller-Christian disease is a chronic multifocal form of Langerhans cell histiocytosis.70% of cases occur between the ages of 2 and 6. The four characteristic clinical findings are bone lesions, diabetes insipidus, exophthalmus, mucocutaneous lesions. Bones lesions are osteolytic and preferentially involve the calvarium.

The joint most frequently affected in acne fulminans is the:
1 Elbow
2 Intervertebral
3 Distal interphalangeal joints of the hand
4 Sternoclavicular
5 Sacroiliac
Sternoclavicular
Acne fulminans may be associated with lytic bone changes which are indicative of a sterile osteomyelitis. The sternoclavicular and chest wall joints are most frequently affected

A 16 year old developmentally normal male presents to his pediatrician intermittent vague epidodes of hand and feet paresthesias and non specific episode of GI distress. He is referred to you to evaluate numerous punctate to 5 slightly verrucous, deep-red to blue-black papules distributed diffusely on his trunk in a bathing suit distribution. Polarization microscopy of the sediment of his urine demonstrates birefringent lipid globules (ie, renal tubular epithelial cells or cell fragments with lipid inclusions) with the characteristic Maltese cross configuration. How is this disorder inherited?
1 Autosomal dominant
2 Autosomal recessive
3 X-linked dominant
4 X-linked recessive
5 Not an inherited disorder
X-linked recessive
Fabry’s disease is inherited is x-linked recessive. Female carriers often exhibit mild forms of this disorder. It can be establish that a patient has FD by searching for low activity of alpha-galactosyl A in plasma, leukocytes, cultured skin fibroblasts, or dried blood spots on filter paper. Because of the Lyon effect, enzymatic detection of carriers can be misleading; thus, specific genetic analysis can be helpful in making the diagnosis.
Since the age of 10 this 28-year-old man has had multiple progressive dark red papules on the lower half of the body associated with episodic heat-triggered acral pain, decreased sweating, dry skin, abdominal pain and an impaired quality of life. He had relatives with chronic burning pain in the extremities, bowel disorders, red purple papules, psychiatric and cardiac diseases. The clinical suspicion of Fabry disease was confirmed with low alpha-galactosidase A activity in blood and a mutation in the alpha-galactosidase A gene. Additional findings included microalbuminuria, perypheral neuropathy, vascular tortuosity in conjunctiva and retina as well as cornea verticilata.. Fabry disease is a rare X-linked disorder caused by deficient activity of the lysosomal enzyme alpha-galactosidase A. Progresive accumulation of the substrate globotriaosylceramide in cells throughout the body leads to major organ failure and premature death. Enzyme replacement therapy with agalsidase alpha leads to significant clinical benefits in patients with Fabry disease, and treatment is likely to alter the natural history of this disorder.

What complication can occur if this disease is left untreated?
1 Development of a squamous cell carcinoma
2 Testicular torsion
3 Erectile dysfunction
4 Impotence
5 Pseudo-ainhum
Development of a squamous cell carcinoma
Lichen sclerosis is most commonly located in the genitalia. Longstanding lichen sclerosis is thought to be a risk factor for the development of a squamous cell carcinoma.
Which enzyme can be a useful adjunct test to diagnose zinc deficiency where the serum zinc level is normal or near normal?
1 Zinc sulfatase
2 Alkaline phosphatase
3 AST
4 ALT
5 Creatinine kinase
Alkaline phosphatase
A low serum alkaline phosphatase, a zinc dependent enzyme, may be a valuable adjuctive test where the serum zinc level is normal or near normal. The diagnosis of zinc deficiency should be suspected in at-risk individuals with acral or periorificial dermatitis. It is usually confirmed by low serum zinc levels.
Which of the following is a feature of Sneddon’s syndrome?
1 Venous thromboses
2 Hepatosplenomegaly
3 anti-Scl-70 autoantibodies
4 M. tuberculosis infection
5 C2 deficiency

Venous thromboses
Sneddon’s syndrome presents as livedo reticularis and livedoid vasculitis associated with ischemic cerebrovascular lesions, hypotension, and extracerebral arterial and venous thromboses.

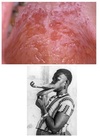
A 25 year-old previously healthy man presents with the skin findings shown, urethritis, and one month of peripheral arthritis. Which of the following is true regarding this condition?
1 Females and males are equally affected
2 A chronic deforming arthritis occurs in 20%
3 TNF-alpha inhibiting agents have no role in the treatment of this condition
4 Patients must have urethritis, conjunctivitis, and arthritis for diagnosis
5 Chlamydia cervicitis is not associated with this condition

A chronic deforming arthritis occurs in 20%
The patient has Reiter’s syndrome. Reiter’s syndrome is a chronic inflammatory disease similar to psoriasis with psoriatic arthritis, and is thought to be a variant form. The classic triad consists of urethritis, conjunctivitis, and arthritis. Few patients present with the classic triad, and thus the syndrome can be diagnosed with peripheral arthritis >1 month duration and associated urethritis (or cervicitis). It occurs in young men with the HLA-B27 genotype and rarely occurs in women. Skin findings include keratoderma blennorrhagicum and circinate balanitis (in men), as well as oral erosions, severe stomatitis, and nail changes. The course of disease is marked by exacerbation and remission; a chronic deforming arthritis occurs in 20%. Treatment includes topical steroids, NSAIDs, methotrexate, acitretin, cyclosporine, and TNF-inhibiting biologics, such as etanercept.
Secondary systemic amyloidosis:
1 Classically involves the tongue and periorbital skin
2 Involves deposition of AL protein
3 Can involve deposition of beta 2-microglobulin in the setting of rheumatoid arthritis
4 Can be noted on biopsy of normal skin
5 Involves deposition of keratin-derived amyloid
Can be noted on biopsy of normal skin
Secondary systemic amyloidosis presents with deposition of amyloid in the adrenals, liver, spleen, and kidney as a result of some chronic disease, such as TB, leprosy, Hodgkin’s, Behcet’s, rheumatoid arthritis, ulcerative colitis, schistosomiasis, or syphilis. The skin is not involved. AA amyloid fibrils, derived from SAA protein (an acute phase reactant) are deposited. AA is also seen in Muckle-Wells and familial mediterranean fever. Biopsy of normal skin may be positive for perivascular amyloid. Dialysis-related amyloidosis occurs via deposition of beta 2-microglobulin component altered by uremia, and resuls in carpal tunnel syndrome, bone cysts, and spondyloarthropathy.