ECGs + Arrhythmias Flashcards
(136 cards)
When is ECG monitoring required?
- Cardiac arrest
- Syncope
- Chest pain
- Persistent arrhythmia
- Shock or other severe illnesses
- Other indications - severe electrolyte disturbances, poisoning, during and after interventions e.g. major surgery
When should you start and stop ECG monitoring in a cardiac arrest?
You should establish cardiac monitoring as soon as possible during cardiac arrest. In many patients who have been resuscitated from cardiac arrest there is a substantial risk of further arrhythmia and cardiac arrest.
It is important to maintain cardiac monitoring in people who have been resuscitated from cardiac arrest until you are confident that the risk of recurrence is very low.
A patient presents to A&E with syncope. Why is a 12-lead ECG indicated in this patient?
Some people experience syncope (transient loss of consciousness due to a reduction in blood supply to the brain) caused by an intermittent cardiac arrhythmia that, if not documented and treated, could lead to cardiac arrest or sudden death. However, the arrhythmia may not still be present at the time of initial assessment.
If a person presents with syncope you should undertake careful clinical assessment and record a 12-lead ECG.
A patient presents to A&E with syncope. You record a 12-lead ECG. In what circumstances is admission and cardiac monitoring NOT necessary?
ECG monitoring and hospital admission are not usually required for people who have experienced:
- uncomplicated (vasovagal) fainting
- situational syncope (e.g. cough syncope or micturition syncope) or
- syncope due to orthostatic hypotension
A patient presents to A&E with syncope. You record a 12-lead ECG. In what circumstances is admission and cardiac monitoring necessary?
Start ECG monitoring and arrange further expert cardiovascular assessment in those patients who have had:
- unexplained syncope, especially during exercise
- syncope and have evidence of structural heart disease
- syncope and have an abnormal ECG (especially a prolonged QT interval).
What type of ECG would you request for a patient admitted to A&E with chest pain?
People experiencing chest pain due to acute coronary syndromes will be at risk of developing a cardiac arrhythmia that may place them at risk of cardiac arrest and death.
Single-lead ECG monitoring is not a reliable technique for detecting evidence of myocardial ischaemia (ST-segment depression). Record serial 12-lead ECGs in people experiencing chest pain suggestive of an acute coronary syndrome.
When is ECG monitoring appropriate for a persistent arrhythmia?
A persistent arrhythmia + SYMPTOMS e.g. hypotension, heart failure
Monitor the ECG (along with other physiological measurements) to identify and respond to deterioration at the earliest possible time.
What are the 3 different types of ECG monitoring?
- In emergency situations such as cardiac arrest, the cardiac rhythm must be assessed as soon as possible. Self-adhesive pads are used for monitoring rhythm and hands-free shock delivery.
- If a patient requires monitoring, but is not so critically ill that defibrillator pads are likely to be needed, 3-lead monitoring is the standard form of ECG monitoring employed by many cardiac monitors and defibrillators in general clinical use.
- The heart is a three-dimensional organ and the 12-lead ECG addresses this by examining the heart’s electrical signals from 12 different directions. In some clinical settings, such as a cardiac care unit, 12-lead monitoring is available to enable early detection of ECG abnormalities that may be seen in a limited number of leads.
If an arrhythmia has been detected by a 3-lead ECG monitor, what further investigation can give you more information about the arrhythmia?
record a 12-lead ECG during an arrhythmia that has been detected by simpler monitoring
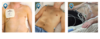
Where are the pads/electrodes placed for a defibrillator and a 3-lead ECG monitor?
- defibrillator - pads should be applied beneath the right clavicle and in the left mid-axillary line, overlying the V6 ECG electrode position. This is also known as the pectoral/apical position and facilitates rapid rhythm assessment and defibrillation. These pads should be applied whilst CPR is in progress with the aim of minimising interruptions in chest compressions.
- 3 lead - the electrodes are placed over the bony parts of the shoulders and that the ‘leg’ electrode is often placed on the lower left chest wall over ribs or costal cartilages, to minimise artefact from underlying muscle
What does the p wave represent?
In normal sinus rhythm, depolarisation begins in pacemaker cells at the sino-atrial (SA) node.
A wave of depolarisation then spreads from the SA node through the atrial myocardium. This is seen on the ECG as the P wave.

What does the P-R interval represent?
When the electrical impulse in the atria reaches the AV node it is conducted slowly, represented on the ECG largely by the isoelectric portion of the PR interval.

What does the QRS complex represent?
The bundle of His carries the Purkinje fibres from the AV node and then divides into right and left bundle branches, spreading out through the right and left ventricles respectively.
Rapid conduction down these fibres ensures that the ventricles contract in a co-ordinated fashion. Depolarisation of the bundle of His, bundle branches and ventricular myocardium is seen on the ECG as the QRS complex.

What is the mechanical response of the heart to the electrical impulse represented by the p wave?
p wave - atrial depolarisation
mechanical response to this = atrial contraction
What is the mechanical response of the heart to the electrical impulse represented by the QRS complex?
QRS complex - ventricular depolarisation
mechanical response to this = ventricular contraction
What is meant by sinus rhythm?
Sinus rhythm
The atria and ventricles are contracting in sequence at the same rate (approximately 60 beats min-1 and myocardial activity is coordinated.

Describe the pathophysiology and management.

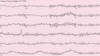
Ventricular fibrillation
The electrical activity is chaotic, there is no coordinated muscle activity in either the atria or ventricles and the pumping action of the heart is lost. Urgent defibrillation is indicated as soon as it is safe to do so and treated according to the ‘shockable’ algorithm.
Describe the pathophysiology and management.

Ventricular tachycardia
The ventricles are contracting at a much faster rate than the atria. There may or may not be a pulse rhythm - confirmation of cardiac arrest will dictate the action taken.
Describe the pathophysiology and management.

Asystole
Neither the atria or ventricles exhibit any electrical or mechanical activity.
- If you cannot see any electrical activity check the patient: are there signs of life?
- If not, then cardiac arrest is confirmed and CPR should be started.
- If electrical activity is present and the patient shows signs of life, then continue with the next steps of rhythm recognition. Be aware that poor electrode contact or placement will affect the ECG trace.
How do you measure
1) PR interval
2) QRS duration
3) QT interval
- PR interval = beginning of p to beginning of q
- QRS duration = beginning of q to end of s
- QT interval = beginning of q to end of t

6-stage approach to interpreting ECG rhythm strips…
- Is there any electrical activity?
- What is the ventricular (QRS) rate?
- Is the QRS rhythm regular or irregular?
- Is the width of the QRS complex normal (narrow) or prolonged (broad)?
- Is atrial activity present?
- Is atrial activity linked to ventricular activity, if so, how?
How do you calculate ventricular rate from an ECG rhythm strip?
number of R-R intervals in 6s (30 big squares) x10
if rhythm strip not long enough,
number of R-R intervals in 3s (15 big squares) x20
What is normal heart rate?
The normal heart rate (ventricular rate) at rest is 60-100 beats min-1
Bradycardia is a heart rate slower than 60 min-1
Tachycardia is a heart rate faster than 100 min-1
How do you work out if the QRS rhythm is regular or irregular? What should you do if it is irregular?
measure out each R-R interval and compare it to others in the rhythm strip
If the QRS rhythm is irregular you will need to decide:
is this totally irregular, with no recognisable pattern of R-R interval?
is the basic rhythm regular, with intermittent irregularity?
is there a recurring cyclical variation in the R-R intervals?