Final Flashcards
(275 cards)
True/False: Inflammation (Ex. Enteritis) leading to Colic will Typically present as Strangulating Disease
True
How to Diagnose Choke
NG Intubation- Inability to Enter Stomach
*Endoscopy- Used to Asses Presence and Extent of Damage to Esophagus but not necessary for Diagnosis

Diagnostic Test used to Confirm Cases of Diaphragmatic Hernias
Ultrasound

Medical Managment that can be used in Patients with Equine Metabolic Syndrome in Horses not responding to Exercise and Diet Strategies
Levothyroxine Sodium
How would Non-Strangulating Small Intestinal Disease Differ from Strangulating Small Intestinal Disease?
Less Cardiovascular Compromise
Variable/Less Reflux
Less Tightly Distended Loops on Rectal Palpation
Typical Clinical Sign in Horses with Dsyuria/Stranguria

Urine Scalding of Hind Limbs

Treatment for Left Dorsal Displacement (LDD) of Large Colon
Medical: IV Phenylephrine -Causes Contraction of the Spleen and Release of Large Colon
Surgery: Ventral Celiotomy- If Phenylephrine does NOT work
*When Done with Phenylephrine Drip, Jog the Horse around for 15 Mintues and then Re-Rectal the Horse

Three Most Useful Indicators of Liver Disease
SHD
GGT
Serum Bile Acids
*In the Face of Significant Liver Disease, at least one of the three will be Elevated

After Gastric Decompression the Horse is in Less Pain. 100 mg Xylazine is Administered. The Mare stays relatively Pain Free for 30 Min. Pain Increases Again and another 9.5 L of Reflux is Obtained. The Mare is Administered another 100 mg of Xylazine which keeps her Comfortable for longer. It is 1 Hour later that she is Refluxed again, 10L reflux Obtained. The Mare is Progressively Depressed. Analysis of the Peritoneal Fluid is Obtained by Abdominocentesis reveals Serosanguinous TP = 4.5 g/dL, WBC = 11,600

What Features of the Case helped Make the Decision for this Diagnosis (Duodenitis Proximal Jejunitis)?
The Rectal Palpation- Moderately Distended Loops
The Abdominocentesis- TP Increased
The Volume of Reflux- Copious Amounts of NG Reflux
The Response to Reflux- Pain Subsides or abates after Decompression, most Horses Remain very Depressed
The Temperature- Rectal Temperature > 101 F
The CRT- Prolonged CRT (> 3 seconds)

Renal Toxicity Described Below:
Most common Cause of Tubular Nephrosis in Horses
Risk of Acute Renal Failure- Increased if concurrent use of NSAIDs, Dehydration, Endotoxemia, Prolonged Administration (> 10 Days)
Clinical Signs- Typically Polyuric, Depression and Anorexia
Aminoglycoside Nephrotoxicity

Free-Flow
*Free-Flow most commonly used- Put new Bedding in Stall

What Drug should be AVOIDED when Treating Liver Disease
Diazepam
*Enhances Effects of GABA on Inhibitory Neurons
*AVOID Diazepam in Horses with Liver Disease

1. The Rectal Palpation- Empty Caudal Abdomen/Reduced Palpable Loops
2. The Abdominocentesis
7. The Progression- Recurrence/Episodic Colic
*Most Diaphragmatic Hernias in the Horse are going to be Large- More than just the Small Intestine will be herniated through the Diaphragm into the Thorax. Will not Feel normal Structures on Rectal Palpation because they are all pushed Forward (Empty)
Three Risk Factors of PRIMARY Non-Strangulating Large Colon Impaction
Teeth- Dental Abnormalities
Winter Season
Water Restriction
*Most Notably will see Primary Non-Strangulating Large Colon Impactions Develop in Winter Months
If horses have Poor Dentition they are going to be Chewing their hay less well and therefore will have larger Fiber Components in their colon which will predispose them to impactions
______ Mechanisms likely MAJOR underlying Cause of Ileus regardless of Initial insult
Inflammatory
*Late stage POI is mainly associated with Inflammatory Mechanisms irregardless of what the underlying cause is

Differential for Small Intestinal Strangulating Disease where the Animal gets Progressively Depressed
DPJ (Anterior Enteritis)

Three Most Common Etiologies leading to Cresty Necked Horses
Hypothyroid
Pituitary Adenoma
Equine Metabolic Syndrome

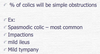
B, C, D, E
*High Levels of Glucose in the Blood leading to Glucosuria

Pathophysiology of which Cause of Colitis:

Obligate Intracellular Parasite which Infects Trematode
Trematode then Infects Snails and many Aquatic Insects
Focus on Fresh Water Snails and Fluke
Inadvertent Ingestion of Aquatic Insects and Snails
Potomac Horse Fever
*Accidental Ingestion of the Infected Trematode Vector- How the Horse Develops Disease- Be Careful with Feed and Water Sources
Most Diagnostic Serum Abnormality in Patients with Hyperlipemia
Serum Triglyceride Levels in Excess of 500mg/dL

NG Reflux: None
Rectal: Very Firm Slightly Indentable Structure in Left Ventral Quadrant. Filled Structure coming across Pelvic Inlet
Abdominocentesis: TP
What is the Likely Diagnosis in this Case?

Large Colon Impaction
*Non-Strangulating Large Intestine
*Normal Abdominocentesis- Common with Non-Strangulating Lesions
Colitis- Inflammatory Disease of the Large Colon that looks STRANGULATING
Large Colon Volvulus = Strangulating
Cecal Impaction- Would be Located in the Right DORSAL Quadrant
On Rectal Palpation, if Kidney is Larger, Softer and Painful it is ____Disease
Acute
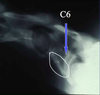
_____ Dorsal Displacement of the Large Colon is also known as Nephrosplenic Entrapment
Left Dorsal Displacement (LDD)
*Large Colon becomes Distended and Filled with Gas. The Colon Migrates up along the Body Wall and hooks into the Nephrosplenic Ligament. Large Colon becomes stuck in the Space because there is a Ledge on the Spleen
*Main Therapy for Left Dorsal Displacement of the Large Colon targets the SPLEEN. Contraction of the Spleen will Minimize the Ledge and the Large Colon will no longer be Entraped


Albuminocytologic Dissociation
*VERY Elevated Protein in the Abscence of Increased WBC