HTC (COMBINED) Flashcards
I combine all topics here, but I also have them seperately. Study all here or sperately by topic names (623 cards)
Odontogenic Cysts can be two types
Inflammatory
or
Developmental
Inflammatory cysts
List ( 4 cysts)
- Periapical (radicular)
- Residual periapical
- Buccal bifurcation
- Paradental
Developmental Cysts
List ( 9 cysts)
‐ Dentigerous
‐ Eruption
‐ Gingival cyst of newborn
‐ Gingival cyst of adult
‐ Lateral periodontal
‐ Glandular odontogenic
‐ Odontogenic keratocyst
‐ Orthokeratinized odontogenic
‐ Calcifying Odontogenic
The following cysts are histologically the same in which way
-Periapical (radicular)
‐ Residual periapical
‐ Buccal bifurcation
‐ Paradental
‐ Dentigerous
‐ Eruption
‐ Gingival cyst of newborn
‐ Gingival cyst of adult
all lined by squamous epithelial
What are the
Sources of epithelium
within the jaw bone
▪ Epithelial rests of Malessez
▪ Reduced enamel epithelium
▪ Fissural cysts – when 2 pieces of bone come together
▪ Odontogenic cysts
▪ Epithelial component of odontogenic tumors
▪ Salivary gland inclusions – rare, incorporated in development
radicular cyst, inflammatory cyst are other names for ?
Periapical Cysts
The most common cyst of the jaws ?
Periapical Cysts
Periapical Cysts
Demographic and location
▪ Any age (peak in 3rd ‐ 6th decades, rare in 1st decade)
▪ No sex predilection
▪ MX > MD (anterior MX most common)
Tooth vitality and Periapical Cysts
- Involved tooth usually non‐vital/non‐responsive with thermal and electric pulp testing
- Should test vitality of tooth if see radiolucency in apex\
- If tooth vital, and still see radiolucency ► should do biopsy
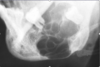
Periapical Cyst
(Radiographic)
- Usually appears as well‐circumscribed periapical radiolucency with widening of the PDL space and/or loss of lamina dura
- Typically small (< 1 cm) but can grow to large dimensions if left untreated
- Radiographic findings can NOT be used for definitive diagnosis
Why the Radiographic findings of Periapical Cyst can NOT be used for definitive diagnosis?
‐ similar appearance with:
- periapical granuloma
- odontogenic tumors
- early COD {Cemento Osseous Dysplasia}
Lateral radicular cyst appears on the lateral surface of the root of a non‐vital/non‐responsive tooth
‐ A differential for which cyst?
lateral periodontal cyst

Periapical Cysts
►Would need to test both teeth for vitality.

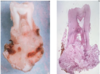
Periapical Cyst

Periapical cyst
shows inflammation at site
abscess developed fistula tract thru
soft tissue. Pt will have pain until
pressure is released
Periapical Cyst
treatment
- endodontic therapy or extraction of involved teeth
- larger lesions may require biopsy along with endodontic therapy
- lesions which fail to resolve should be biopsied
- follow-up at 1-2 years
Residual Cyst
Etiology
- After tooth extracted, not properly cleaned ► the residual cells of the cyst lining and inflammatory cells continue to proliferate
- Has to be at site where tooth was previously removed
Residual Cyst
Radigraphically
- well defined round to oval radiolucency in the site of a previous extraction
Residual Cyst
Histologically is identical to which cyst?
- identical to the radicular cyst (periapical cyst)
- Should biopsy to rule out other causes
Residual Cyst
Treatment
-Removal
- Enucleation if small
- Marsupialization if large
- Note:*
- Enucleation* means: removal of an organ or other mass intact from its supporting tissues
Marsupialization means: surgical technique of cutting a slit into an abscess or cyst to empty its contents and suturing the edges of the slit to form a continuous surface from the exterior surface to the interior surface of the cyst or abscess.
Promotes Decompressing and shrinkage.

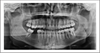
Residual Cysts

Residual Cyst
Paradental Cyst
Etiology
Some controversy over this designation
‐ some think they are inflammatory cyst
‐ some think they are developmental cysts
▪ Etiology: remains unclear
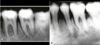
Paradental Cyst
Radiographically
- Radiolucent area noted
- most frequently, along the distal aspect of an impacted or partially erupted third molar