Intracellular Accumulations and Pathologic Calcifications Flashcards
(43 cards)
1
Q
4 Main Pathways of Cellular Accumulation
A
- Abnormal Metabolism (Steatosis/Fatty Liver)
- Defect in Protein Folding/Transport (Mutated forms of alpha 1 anti trypsin)
- Lack of Enzyme (Storage Disorders)
- Ingestion of Indigestible Materials (Carbon/Silica)
2
Q
Steatosis/Fatty Change
A
- Abnormal accumulation of triglycerides within parenchymal cells
- Liver (main), heart, muscle, kidneys
- caused by: toxins, protein malnutrition, diabetes mellitus, obesity, anoxia, alcoholic liver disease
3
Q

A
Steatosis
4
Q
Cholesterol and Cholesterol Esters
A
- metabolism tightle regulated
- used for synthesis of cell membranes
- no intracellular communication
- will see intracytoplasmic vacuoles if accumulated
5
Q
Atherosclerosis
A
- Smooth muscle cells and macrophages in surface/wall of arteries filled with lipid vacuoles
- mostly cholesterol and cholesterol esters
- Aggregates of foam cell in surface/wall give yellow appearance of atheromas
- some may rupture releasing lipids into extracellular space
- will see cholesterol clefts-cholesterol esters crystallized as long needles
6
Q

A
Atherosclerotic lesion
7
Q
Xanthomas
A
- intracellular accumulation of cholesterol
- Xanthomas=groups of foamy macrophages found in connective tissue of skin and in tendons
- can be seen in non hyperlipidemic states
8
Q
A
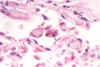
Gastric Xanthoma
9
Q

A
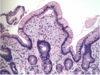
Cholesterolosis of Gallbladder
10
Q
Neimann-Pick Disease, Type C
A
- lysosomal storage disease
- mutations in enzyme involved in cholesterol trafficking
- cholesterol accumulates in multiple organs
11
Q
Renal Tubule Reabsorption Droplets
A
- Seen in kidney conditions that have protein loss in the urine
- increased reabsorption of protein into vessicles
- protein has a appearance of pink hyaline droplets within cytoplasm of proximal tubular cells
- reversible
12
Q

A
Renal tubule reabsorption droplets
13
Q
Russel bodies
A
- plasma cells actively synthesizing immunoglobulins may show russel bodies
- ER becomes hugely distended: large eosinophilic cytoplasmic inclusions
14
Q

A
Russel bodies
15
Q
Alpha 1 anti trypsin deficiency
A
- mutation in protein slows protein folding
- causes build up of partially folded intermediates that aggregate in liver cells
- resulting deficiency causes emphysema of the lungs
16
Q

A
Alpha 1 anti trypsin deficiency
17
Q
Accumulation of cytoskeletal proteins
A
- certain injuries cause aggregation of keratin filaments and neurofilaments
18
Q
Alcoholic Hyaline (Mallory Denk body)
A
- eosinophilic cytoplasmic inclusion in liver cells
- composed of keratin intermediate filaments
- characteristic of alcoholic liver disease
19
Q

A
Mallory Denk Body
20
Q
Neurofibrillary tangle
A
- Found in alzheimers
- neurofilaments and other proteins
21
Q

A
Neurofibrillary tangle
22
Q
Hyaline
A
- descriptive term
- alteration of cellular or extracellular space that gives homogenous glassy pink appearance on routine H&E
23
Q

A
Arteriolar Hyaline
24
Q
Glycogen
A
- Stored in cytoplasm
- excessive deposits with problem in metabolism
- diabetes is most important disease in glucose metabolism
- accumulations appear clear
- Pompe disease, von Gierke disease
25

* normal glycogen on squamous epithelium
26
Carbon (Exoegnous)
* inhaled, picked up by alveolar macrophages, transported through lymphatic channels to regional lymph nodes
* blackens lungs and node tissues "anthracosis"
* coal miners may get serious lung disease
27

Coal dust/anthracosis
28
Tattoo (Exogenous)
* skin is phagocytosed by dermal macrophages
* inert, not associated with inflammation
29

Bowel tattoo in surgery
30
Lipofuscin
* wear and tear pigment
* seen in liver and heart of aging or malnutrition cancer cachexia
* insoluble polymers of lipids and phospholipids in complex with proteins derived from breakdown of subcellular membranes
* not harmful to cells
* may indicate cell exposure to free radical injury
31

* Lipofuscin pigment
32
Melanin (Endogenous)
* formed when tyrosinase catalyzes the oxidation of tyrosine to dihydroxyphenylalanine in melanocytes
33

Melanin
34
Normal vs excess iron breakdown
* normal: in sites where there is red blood cell breakdown
* local excess: macrophages breakdown blood. removal of iron--\>ferritin--\>hemosiderin
* parallel breakdown of heme moeity: biliverdin--\>bilirubin
* bruising colors
35
Iron metabolism
* Iron is normally carried by transferrin, stored by apoferritin in cells, forms ferritin micelles (normal)
* excess iron, ferritin forms excess hemosiderin granules (aggregates of ferritin micelles) in cells
36
Hemosiderosis
* systemic overload of iron--\>hemosiderin buildup in tissues
* Causes: increased absorption of dietary iron (hemachromatosis)
* hemolytic anemias(premature lysis of RBC's, excess release of iron)
* repeated blood transfusions (equivalent to exogenous administration of iron)
37

Hemosiderosis in liver from hemochromatosis
38
Dystrophic Calcification
* deposits of calcium in dying tissue (necrosis)
* present in atheromas of advanced atherosclerosis
* aging, damaged heart valves
* psammoma bodies, asbestos bodies
39

Calcification of cardiac valves
40

Psammoma bodies
41
Asbestos bodies
42
Metastatic calcification
* Deposition in normal tissues where there is hypercalcemia
* 1. Increased secretion of parathyroid hormone (PTH) with subsequent bone resorbtion (e.g. due to parathyroid tumors)
* 2. Resorbtion of bone (tumors: myeloma, leukemia, extensive
* skeletal metastases; accelerated turnover–Paget’s disease; immobilization)
3. Vitamin D related disorders (Vit D intoxication, sarcoidosis)
* 4. Renal failure (Renal failure--\>retention of phosphate--\>
hyperparathyroidism)
* Other: mild-alkali syndrome (excessive ingestion of calcium and
absorbable antacids e.g. mild or calcium phosphate)
43
Where does metastatic calcification occur?
* throughout body
* gastric mucosa, kidneys, lungs
* these secrete acid --\>have alkaline compartment predisposed to calcification
* usually no clinical dysfunction unless massive deposition in lungs , kidneys
