Lungs & Pleurae Flashcards
(31 cards)
What are the 3 throacic compartments & what are they enclosed by?
- pulmonary cavities are enclosed by pleurae
- serous membrane of throacic cavity; parietal & visceral continuous at root of lung
- parietal pleura: lines inner surface of thoracic cavity
- visceral pleura: covers lungs
-
pleural cavity = potential space between them w/ small amount of pleural fluid
- reduce friction (when breathing)
- create surface tension through fluid bond btw visceral & parietal layers
- so when thoracic wall moves, the lung is draged along with it
- Right pulmonary cavity
- lungs
- left pulmonary cavity
- lungs
- mediastinum
- separates R & L pulmonary cavities
- has heart & great vessels

What is a pneumothorax? different types?
- pneumothorax = presence of gas in pleural space
- changes pressure gradient & lung collapse
- with regular pneumothorax, there is puncture of the parietal pleura & air is able to escape leaving an “empty” pleural cavity at atmospheric pressure
- with tension phenumothorax air cannot escape, so prellure starts to increase which places a lot of pressure on mediastinal structure & can cause cardiac shift

What are the 4 continuous parts of the Parietal pleura?
- costal
- lines internal surface of thoracic wall
- endothoracic fascia
- lines internal surface of thoracic wall
- diaphragmatic
- lines superior surface of diaphragm
- mediastial
- lines lateral aspect of mediastinum
- cervical
- covers apes, extends inot root of neck
- suprapleural membrane
- covers apes, extends inot root of neck

What are the pleural recesses & why do they exist?
the lungs do not fill the entirity of hte pulmonary cavity, so the lunge & parietal pleura have different boundaries, which yields spaces within the pleural cavity
- costomediastinal recesses
- posterior to sternum
- bilaterally asymmetric due to heart
- costodiaphragmatic recess
- where costy & diaphragmstic pleura meet up
- size variable with phase of respiration
- inspiration: smaller b/c lung fill it more
- exhallation: larger as lung moves superiorly
- prone to fluid accumulation in upright position

What is the name for abnormal accumulatin fo fluid int he pleural space?
pleural effusion
- common causes: congestive heart failure & malignancy
- small amounts of fluids can be absorbed my lymph, but larger amounts can require thoracentesis (surgical aspiration of the fluid)

-
apex lung = cervical portion parietal pleura
- extend a couple centimeters above the clavicle
- bilaterally descends toward sternal line obliquely
- right parietal pleura follows sterunum and moves l_aterally at 6th rib_
- left parietal pleura follows sternum and moves laterally at 4th costal cartilage to accomidate heart and pericardium
- bilaterally reach mid clavicular line at 8th costal cartilage
- bilaterally reach mid axillary line at 10th rib
- inferior margin of parietal pleura by scapular line is at 11th rib
- paravertebral line, the pleura is inferior to neck of the 12th rib
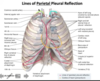
What is the general rule fot he difference in location betweenthe lung margins and pleural lines?
- lungs are ~2 ribs superior at MCL, MAL, PVL
- MCL at 8 : lungs at 6
- MAL at 10 : lungs at 8
- PVL at 12 : lungs at 10
Arterial and venous supply of the costal, diaphragmstic & mediastinal pleura?
- costal part
- intercostal arteries
- diaphragmatic part
- superior phrenic artery + internal thoracic artery
- from aorta or 10th intercostal
- superior phrenic artery + internal thoracic artery
- mediastinal part
- internal thoracic artery
- venous drainage of parietal pleura parallels the arteries
Vasculature of visceral pleura?
- bronchial vessels
- plumonary vessels

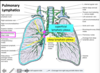
Describe the lymphatic drainage patterns for parietal and visceral pleura
- parietal
- lymphatics drain into adjacent lymph nodes
- costal: intercostal and parasternal lymph nodes
- diaphragmatic: phrenic lymph nodes
- mediastinal: anterior and posterior mediastinal lymph nodes
- all of these eventually drain to the thoracic duct
- lymphatics drain into adjacent lymph nodes
- visceral
- lymphatics drain into the superficial (subpleural) lymphatic plexus of the lungs
- drai to bronchopulmonary nodes
- lymphatics drain into the superficial (subpleural) lymphatic plexus of the lungs
innervation of the pleura?
- parietal - sensitive to pressure, pain, temperature and well localized
- intercostal nerve
- cervical, costal & outer edge dipahragmatic pluera including costodiaphragmatic recess
- phrenic nerve
- medial portion of diaphramatic pleura
- between pericardium and lungs to reach the diaphragm
- intercostal nerve
- nerves (pulmonary plexus) - not sensitive to pain or touch, only stretch
- visceral pleura
Identify the indicated features of the lungs

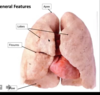
Idenfity the indicated surfaces & borders of the lung

Surfaces are neme for the structures they contact through the
pleura
- costal
- contacts pleura near thoracic wall
- daphragmatic surface
- base of lung
- mediastinal surface
- hilum of lung & slightly concave
- anterior border
- costal and mediastinal surfaces meet up
- sharp - into costal mediastinal recess
- inferior border
- costal and diaphragmatic surfaces meet up
- goes into costaldiaphragmatic recess
- posterior border
- costal and mediastinal surface meet up
- rounded - in paravertebral gutter
*

What are the contents of the root of the lung?
- Bronchi
- contained within the pulmonary sleeve (ligament)
- pulmonary A/V
- vein taking newly oxygenated blood toward the heart
- artery taking oxygen poor blood from heart to lungs
- Bronchial A/V
- nerves
- lymphatics
- pulmonary A/V
Hilum = area
root = contents (at the hilum)
What is the relationship between the contents within the hilum of the lung?
-
bronchus is most posterior
- thick, cartilageous walls
-
inferior pulmonary vein is most inferior structure
- superior pulmonary vein is slightly anterior to inferior pulmonary vein
- the rest should be arteries
- generally will be more superior than the veins

Identify the medial relations indicated in the provided image

*

Identify the features of the right lung


Identify the features of the left lung


At what landmark levels can you find the fissures of the lungs? How is this helpful?
- Oblique fissures (both lungs)
- start at T4
- wrap around anteriorly at MAL (5th rib)
- continue anteriorly to level of 6th costal cartilate
- horizonatal fissure (right lung only)
- starts level 5th rib MAL
- wraps around anteriorly following 4th rib to ternum
- to auscultate the middle lobe of the right lung, need to stay anteriorly between the 4th adn 6th rib
Describe the basics of ventilation
- lungs rely on external muscles, expandable thoracic cage & Boyle’s Law for respiration
-
Inspiration:
- __active process, diaphragm contracts + descends, intercostal mm elevate the ris, intrapulmonary pressure decreases, allowing air to expand the lungs
-
Expiration
- passive process, diaphragm relaxes + rises, lungs recoil and compress alveoli, pressur increases, air is expelled
- Dependent on normal elasticity of healthy lungs
Describe the strucutre of the tracheobronchial tree
- below the larynx is the tracheobronchial tree
- tracheobronchial tree
- cartilaginous rings- keep it open
- muscle- control airflow
- mucosal lining- glands to secrete fluid, cilia to help sweep out foreign objects
- opening posterior
- as we go down the tree, have less cartilage & increased smooth muscle
- trachea ends at T4, leading to primary bronchi

What is the difference between the trajectory of the right and left primary bronchi?
What is the name of the area of bifurcation?
- right primary bronchus is wider & has more of a vertical trajectory
- more prone to aspiration
- goes under they azygous vein
- superior and anterior to right pulmonary artery
- left primary bronchus is less wide and has a left/lateral trajectory
- under aortic arch
- passing anteriorly to esophagus and thoracic aorta
- carina is where bifurcation occurs

Describe how the primary bronchi split as they enter the lungs
-
Primary bronchi
- split into lobar bronchi
- 3 on the right, 2 on the left & named for the lobe they supply
-
lobar split into segmental bronchi that will supply bronchopulmonary segments
- 10 or so in right
- 8-10 in left
- separated by fibrous septa
- important for infection can isolate
-
segmental bronchi subdivide becoming bronchioles
-
terminal bronchiles mark the end of the conduction zone & form respiratory bronchioles
- respiratory bronchioles participat in gas exchagne & lead into alveolar sacs & alveoli
-
terminal bronchiles mark the end of the conduction zone & form respiratory bronchioles
- split into lobar bronchi
Describe the two types pulmonary vasculature
-
pulmonary vessels: gas exchange
- arteries
- arise from right ventricle of the heart
- bifurcate at level of T5, just left of aortic arch
- right passes behind the aortic arch and superior vena cava to enter hilum of right lung
- left passes left of the aortic arch to enter the hilum of the left lung
- arteries branch with the bronchi
- where a pulmonary embolism can occur
- segment is profused with air instead of blood
- most associated with DVT
- end as pulmonary capillaries in the alveolar walls
- now that blood is oxygenated
- From alveolar capillaries, blood drains to tributaries of the pulmonary veins that evenutally dup into one of 4 pulmonary veins
- veins have a peripheral position in the bronchi
- usually superior & inferior will enter separately through the hilum
- right veins pass posteriorly to the right atrium & superior vena cava
- left pass anterior to descending aorta
- dump into right atrium
- arteries
-
bronchial vessels: systemic, supply lungs
- arteries
- at root, you can find them on the posterior surface of the bronchi
- left superior & inferior arteries off the thoracic aorta
-
right is variable
- can come off aorta, 3rd posterior intercostal, left superior broncial artery
- veins
- drains proximal tisues supplied by bronchial artery
- pulmonary veins drain remaining
- arteries