Male gonad disorders Flashcards
(25 cards)
Know the clinical presentations of male hypogonadism (neonatal, teen, adult)
Neonatal: ambiguous genitalia. Child/puberty: delayed puberty. Adult: delayed puberty, delayed growth spurt, sparse chest/pubic/axillary hair growth, erectile dysfunction and/or poor libido, gynecomastia, osteoporosis and fractures, infertility, poor muscle development, hip fat
Know questions to ask on Past History in a patient with hypogonadism
known ambiguous genitalia, undescended testes; mumps orchitis or testicular trauma; prior radiation, chemotherapy; chronic childhood disease (can lead to delay); fam Hx of delayed development or male gonadal abnormalities; did you go through puberty
Know the reversible and irreversible effects of testosterone
Reversible: Libido, spontaneous erections, Male pattern hair growth, Bone mass, Changes in blood proteins (T stimulates erythropoiesis), Sebaceous glands, Sperm production, Muscle strength and size, Prostate and seminal vesicle size, Testes size. Irreversible: Deep voice (laryngeal hypertrophy), Male sexual orientation, Penis size, Body proportions, Baldness, Linear height
5a reductase abnormality
Enzyme that converts T to DHT. Needed to develop external genitalia, prostate, facial and body hair
Know how to investigate male hypogonadism
Lab tests needed. Test T and LH and maybe Prl
Know the causes of primary male hypogonadism and the expected hormonal abnormalities
aka testicular failure. Lab: low T, high LH/FSH. Testicular damage: mumps, trauma, radiation, chemotherapy, drugs; Genetic diseases eg Klinefelter’s syndrome; Sequelae of developmental abnormalities eg undescended testes
Know the causes of secondary male hypogonadism and the expected hormonal abnormalities
aka Hypothalamic/Pituitary Failure. Lab: low T, normal/low LH. Kallmann’s syndrome (LHRH deficiency); Aging (declining LHRH signals with age), “andropause” or ADAM (Androgen Decline in the Aging Male); Pituitary destruction eg tumors, surgery; Increased prolactin (drugs, pituitary tumors); Systemic disease – protective mechanism (ie this isn’t a priority right now!)
Example diagnoses
22yo w/ low T, high LH/FSH, normal prolactin - Most likely Dx: Klinefelter’s syndrome. How to confirm? karyotype Most likely diagnosis if LH/FSH were normal: Kallmann’s syndrome (low LHRH). Most likely diagnosis if he were 16-18 years old: delayed puberty
Know the treatment options for testosterone replacement
Oral: 17alpha alkylated testosterones, T undecanoate (Andriol). I.M.: T enanthate and cypionate. Topical: Patches - Androderm; Gels - AndroGel, Testim, Axiron
Know the adverse effects of testosterone therapy and how to monitor a patient on therapy
ALL androgens in supraphysiological doses may cause: Polycythemia (stimulate erythropoiesis: decreased hepcidin, increased EPO [?]) - stroke; Decrease HDL cholesterol. 17alpha alkylated oral androgens: do NOT use for hypogonadism therapy; may cause cholestatic jaundice, peliosis of liver (blood filled cysts), liver carcinoma (?).
What conditions can T therapy not change?
can’t change testes/penis size or infertility if it wasn’t around for the developmental/puberty years
Know the mechanism of gynecomastia
Imbalance of estrogen/testosterone ratio.
Know the causes of gynecomastia (lots!)
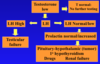
Drugs - testosterone excess (abuse - excess gets converted to E.), digitalis (some plant), prolactin-stimulating drugs, estrogens, substance abuse (marijuana, amphetamines, heroin), herbs/health products; Environmental estrogens/phytoestrogens; Hypogonadism (low testosterone – testicular or hypothalamic/pituitary); Pubertal (common but mild and usually regresses); Hyperthyroid (increased aromatase); Liver cirrhosis (liver supposed to destroy excess E); Genetic defects; Refeeding gynecomastia (malnourished who then eat - axis was thrown off); Testicular cancer (hCG from tumor stimulates T and E production, E>T); Aromatase increase (increased T to E2 conversion)
Know the lab tests done to investigate gynecomastia
Testosterone, Estradiol, Prl, TSH, LH, ß hCG.
Testicular cancer
Common in younger men. Detected with high hCG, often higher estradiol and gynecomastia. hCG binds to testicular LH receptors, stimulating T and E2 synthesis
Know the mechanism of erectile function
Can be: declining hypothalamic GnRH with age; increasing SHBG; increasing sensitivity of hypothalamus to T feedback (ie tolerates low T). No ejaculatory disorder, Very infrequent nocturnal erections, Desire (libido) poor, No performance anxiety
Know the causes of erectile dysfunction
Drugs – antihypertensives, antidepressants (SSRIs – not bupriopion), dopaminergic, alcohol; Neurovascular – diabetes, vascular disease, chronic systemic disease, multiple sclerosis, other nerve injuries; Psychiatric; Testosterone deficiency (not as common)
Know the effects of narcotics for pain on hypothalamic –pituitary-gonadal function
All men receiving narcotics at any dosage should have testosterone measured, as 2/3 have low T; Mechanism: narcotics interact with hypothalamic neurotransmitters to decrease GnRH release, and also interfere with libido; Hypogonadal symptoms do not predict who has low T (chronic pain itself causes poor libido)
Physical findings that are associated with ED
Fine wrinkling around eyes, mouth; Decreased body hair; Pale skin; Testes normal (he thinks they might be slightly smaller); Neuro: mild sensory peripheral neuropathy (diabetes); Cardiovascular: decreased foot pulses; elevated BMI
Nonhormonal contributors to ED
alcoholism, diabetes (neurovascular), vascular
Effects of obesity on T measurements
Obesity lowers SHBGm so “total serum testosterone” measurements will be artificially low. COMMONEST diagnostic problem/error in practice. Need to measure “free testosterone” or “bioavailable testosterone”, Bioavailable T probably best to separate SHBG effects
What other conditions have low levels of T?
Obesity, diabetes, hypertension, hyperlipidemia. But this might not be actually true - did they test total T or bioavailable??
Know the effects of testosterone therapy on a hypogonadal patient and the dose response effects of testosterone
Aim for mid-normal range. There is a dose response to T in muscle, lower fat, but not others. If someone is truly hypogonadal, benefits include muscle, strength, lower fat, mood, sexual function, bone density. Risks? Maybe prostate cancer or benign prostate hypertrophy. No short term problems.
Followup with T therapy in men over 45
Yearly prostate exam, test hematocrit (may increase), lipid levels may change.
