Mitral Valve Disease Flashcards
(63 cards)
mitral valve
- discuss its anatomical structure and location in the heart.
- under physiological conditions - when is it open and how wide does it open?
-
structure: a bicuspid valve made of 2 leafelets
- its opening is enclosed by a fibrous ring
- its leafelets are anchored by chordae tendinae to papillary muscles on the left ventricular wall
- location: in beween the LA and LV
-
open: during diastole
- this allows for filling of the left ventricle
- normally opens to a cross sectional area of 4-6 cm2
- cross sectional area of mitral valve
- what is normal?
- when do we start to see blood flow impairment?
- when does the valvular area become “critical”?
- how do we determine this area?
- normal cross sectional area: 4-6 cm2
- blood flow impairment seen at < 2 cm2
- symptoms start to present at this area
- valve area becomes critical < 1 cm2
cross sectional area determined with echocardiogram.
what is mitral stenosis?
decreased pliability of the mitral valve leafelets that impedes blood flow from the LA to LV
what are the major causes of mitral stenosis?
- rheumatic fever - #1 cause
- congenital
- aging with annular severe calcification
- SLE (lupus)
- RA (rheumatoid arthritis)
discuss the etiology of rheumatic fever
- what sex/demographics does it effect most
- what valvular diseases can it lead to
- # 1 cause of mitral stenosis worldwide
- 40% of valvuar manifestations of RF are mitral stenosis, and the remainder are mitral regurgitation or aortic valve disease.
- theses valvular manifestations usually present a few years - 20 years after initial infection
- 40% of valvuar manifestations of RF are mitral stenosis, and the remainder are mitral regurgitation or aortic valve disease.
- demographics: most prevalent developing countries
- sex: seen more in females > males
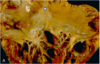
- discuss the major gross morphological changes seen in rheumatic valvular disease?
- what changes are characteristic of early vs end stage rheumatic valve disease?
i believe these are referring to changes in the mitral valve*
- major changes:
- thickening of valve leaflets
- fusion of comissures
- chorda tendinae shortening/thickening
- stage-specific features:
-
early
- leafelets flap open in a “curved over” manner due to restriction of motion at their tips.
- this causes an opening snap on ascultation
- leafelets flap open in a “curved over” manner due to restriction of motion at their tips.
-
as diease progresses:
- symmetric fusion of comissures results in a small, central oval orifice during diastole
-
end stage:
- leafelets can be so fibrotic/stiff they cannot open/shut
-
early
pathogenesis of rheumatic valve disease
it is an abrnomal immune response to group A streptococcal pharyngitis
what criteria must be met to diagnose rheumatic valve disease
- must see 2 major criteria OR 1 major + 2 minor criteria
- major criteria
- carditis
- polyarthritis
- erythema migratorum
- subcutaneous nodules
- chorea (uncontrolled movement)
- minor criteria
- fever
- arthralgia
- previous rheumatic fever/known rheumatic heart disease
- major criteria
what clinical presentations might indicate carditis?
- pleuritic chest pain
- friction rub
- heart failure
carditis is one of the major criteria for dx of rheumatic valve disease
what valves are most/least likely to be effected by rhuematic valve disease
- most likely = mitral/aortic valve
- least likely = pulmonic valve
what physiological changes are seen in mitral stenosis
- mitral stenosis = impaired flow from LA to LV during diastole. blood backs up in LA, doesn’t make it to LV. this leads to:
- LA pressure increase
- LA enlargement
- LV filling dimished
- this decreases end diastolic volume (preload) –> decreases stroke volume –> thus decreases cardiac output
- (CO = HR x SV)
- this decreases end diastolic volume (preload) –> decreases stroke volume –> thus decreases cardiac output

clinical presentation of mitral stenosis
- mild vs moderate
- mild stenosis = typically asymptomatic
- moderate stenosis (valve area 1-2 cm2) = exertional dyspnea and fatigue
- other clinical manifestations:
- chest pain
- atrial fibrillation/palpatitations
- stroke (18 x higher risk in these pts)
- right sided heart failure
- presents w/ edema, ascities, liver failure
- hoarseness (ortner’s dynrome)
- dysphagia
- hemoptysis from ruptured bronchial veins
what two cinical manifestations of mitral stenosis are due to LA enlargement?
- orntner’s syndrome: hoarseness due to the LA enlarging and putting pressure on the recurrent laryngeal nerve
- dysphagia: trouble swallowing due to LA enlarging and impinging on the esophagus
what kind of heart failure is seen in mitral stenosis & why?
what other clinical manifestations typically present alongside this heart failure?
- right sided heart failure
- blood back up into LA backs up into lung and then creates a huge afterload that the right heart must overcome.
- right sided HF can present with:
- edema*
- JDV*
- ascites
- liver failure
discuss key exam findings indicative of mitral stenosis
- what sounds will heard on ascultation?
- other findings
- ascultation
-
murmurs/sounds:
- loud S1 (mitral valve closure)
- opening snap (mitral valve opening) after S2 (aortic valve closure)
-
low-pitched diastolic flow murmur
- caused by turbulent blood flow thru valve
- i_rregular heart rhythm_
-
murmurs/sounds:
- other findings:
- signs of right sided heart failure
- periperal edema
- JVD
- stroke symptoms:
- facial drooping
- weakness on one side of the body
- signs of right sided heart failure
define the clinical significance of the “opening snap” heard on ascultation of a pt with mitral stenosis
- opening snap
- often heard in the early phase of rheumatic valve diease
- this sound is caused by the restriced motion of the diseased valve leafelets during mitral valve opening, which occurs after S2 (aortic valve closure)
- the shorter the interval between S2 and the “opening snap” the more severe the mitral stenosis
label these components of a stethoscope. what is purpose/proper orientation of each component


- when ausculating a patient with possible mitral stenosis
- what part of the stethoscope should you listen with and where on the heart should you place it?
- how should the patient be positioned?
- listen to apex of heart with the bell of the stethoscope
- place patient in left lateral decubitus
what is the “standard” diagnostic test for mitral stenosis
echocardiogram
echocardiogram for dx of mitral stenosis
- what types of echocardiograms can be done and in what circumstances?
- what can an echocardiogram tell you?
- echocardiogram = standard diagnostic test for mitral stenosis
- two possible views:
- transthoracic - usually preferred
- transesophageal (TEE) - preferred when 1. it is difficult to view valves or 2. we’re assessing for vegetations/thrombus
- echocardiogram is key to tell you:
-
degree of stenosis
- mild: mitral valve area > 1.75 cm2
- moderate: mitral valve 1.25 -1.75 cm2
- severe: mitral valve < 1.0 cm2
- pressures across valves/heart chambers
-
degree of stenosis
- two possible views:
other than an echocardiogram - what other diagnostics tests can be done to assess mitral stenosis and under what circumstances?
- EKG - useful if there is an irregular rhythm. could show
- LA enlargement
- right axis deviation
- RBBB
- cardiac catheterization - used if echocardiogram is undiagnostic. can tell you pressure in LA/LV
- exercise test stress - to induce exertional symptoms
when to do a cardiac catheterization in diagnosis of mitral stenosis/what can it tell you?
- do if echocardiogram is diagnostic
- can tell you pressure of LA/LV
when do an EKG if the diagnosis of mitral stenosis/what it can tell you
- do if there is an i_rregular rhythm_
- can show:
- LA enlargement
- right axis deviation
- RBBB
how to treat asymptomatic mitral stenosis
- generally, no treatment.
- unless:
- there is severe pulmonary artery HTN OR new onset atrial fibrillation, in which case:
- control HR with beta blocker/CCB
- and give warfarin (anti-coagulant) if their INR is 2-3
- they need a percutaneous balloon mitral valveotomy
- there is severe pulmonary artery HTN OR new onset atrial fibrillation, in which case: