Muscle fibres comprise of several hundred ….
Myofibrils
Define syncytium
a single cell or cytoplasmic mass containing several nuclei, formed by fusion of cells or by division of nuclei
Features of a muscle fibres
Lipid droplets - fuel for respiration
Nuclei found in periphery of fibre
Lots of mito - high rate of resp
Compare cardiac muscle to skeletal muscle
Cardiomyocytes form shorter fibres than skeletal muscle fibres
Cardiac muscle not built of syncytial fibres; they consist of single cells
Cardiac muscle contains single mono/dinucleated cells with limb-like extensions that allow the cells to connect to each other via intercalated discs
Centrally located nuclei in cardiac muscle; peripheral nuclei in muscle fibres
More mitochondria/capillaries in cardiomyocytes
Describe the length-tension relationship briefly
Amount of force exerted by a sarcomere depends on the degree of overlap between the thick and thin filaments
At full stretch , few myosin heads can attach to actin so the force exerted is weak
Beyond full contraction, the ends of the thin filament get in the way of each other and thick filaments are forced against the Z lines so force is reduced
At optimal length, all myosin head have access to actin so force is maximal
Structure of the fibres in heart walls
Muscle fibres arranged in several directions to achieve spiral like formation which allows the ventricles to contract in a wringing motion
What are intercalated discs?
Connections between cardiomyocytes
Appear as dark jagged lines due to desmosomes
Skeletal muscle fibres have gap junctions
True or false
False
Features of intercalated discs
Desmosomes allow longitudinal force transfer due to their strong adherence
Low resistance gap functions allow fast transfer of APs
strong adherence between fibres
Arrangement of myosin heads in skeletal/cardiac muscle
Antiparallel all the way around the axis

Arrangement of myosin heads in smooth muscle
Antiparallel at opposite sides

Why is the arrangement of myosin heads in smooth muscles advantageous ?
Allows longer sliding distances compared to skeletal muscle
higher amount of contraction can occur
Structure of smooth muscle
Contraction shortens the smooth muscle cell to a fraction of its length while making it thicker
3D network of myosin, actin and intermediate filaments (not sarcomeres)
actin filaments held together by cytoskeletal proteins called dense bodies
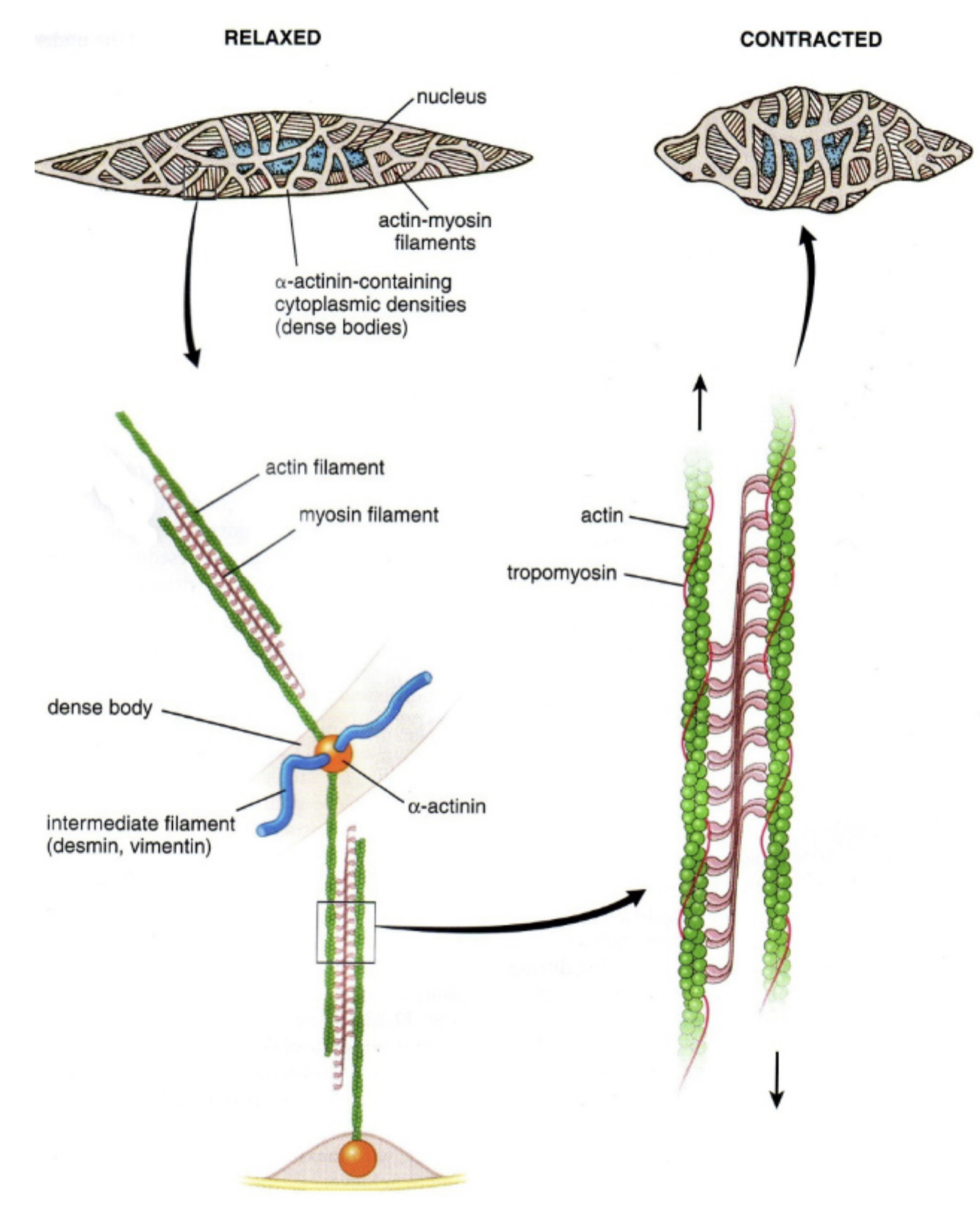
Smooth muscle cell features
Mononucleated
spindle shape
( dense network of filaments with one nucleus in the middle )

Compare the three muscle types

How does striation of skeletal muscle occur
Intermediate filaments such as desmin link Z lines laterally and myofibrils longitudinally
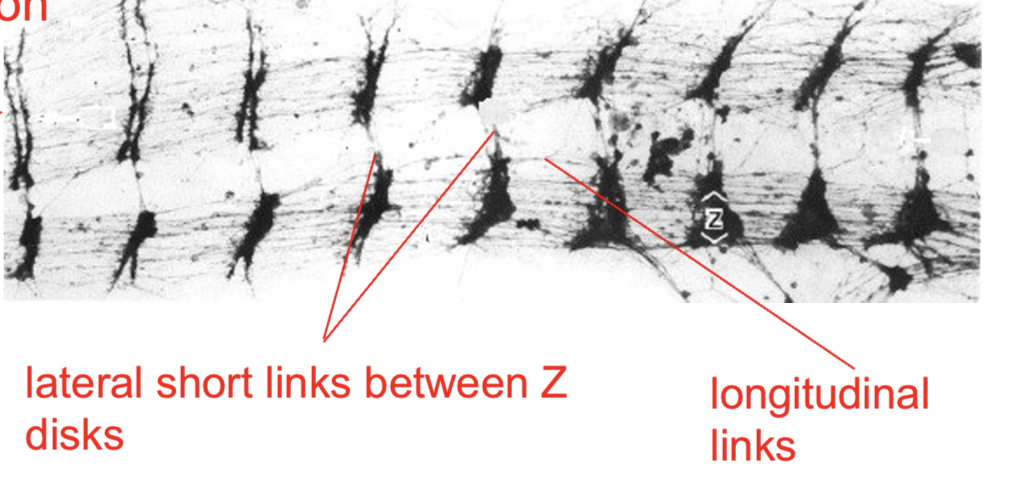
Z lines are laterally linked by
Desmin intermediate filaments
What proteins is mainly responsible for preventing overstretch in muscles ?
Titin
Role of myofibril cytoskeleton
Composed of mainly desmin fibres
Links myofibrils to each other
links synctycia to the basement membrane and into the surrounding connective tissue at the periphery
this allows force of contraction ti be transmitted both longitudinally and laterally
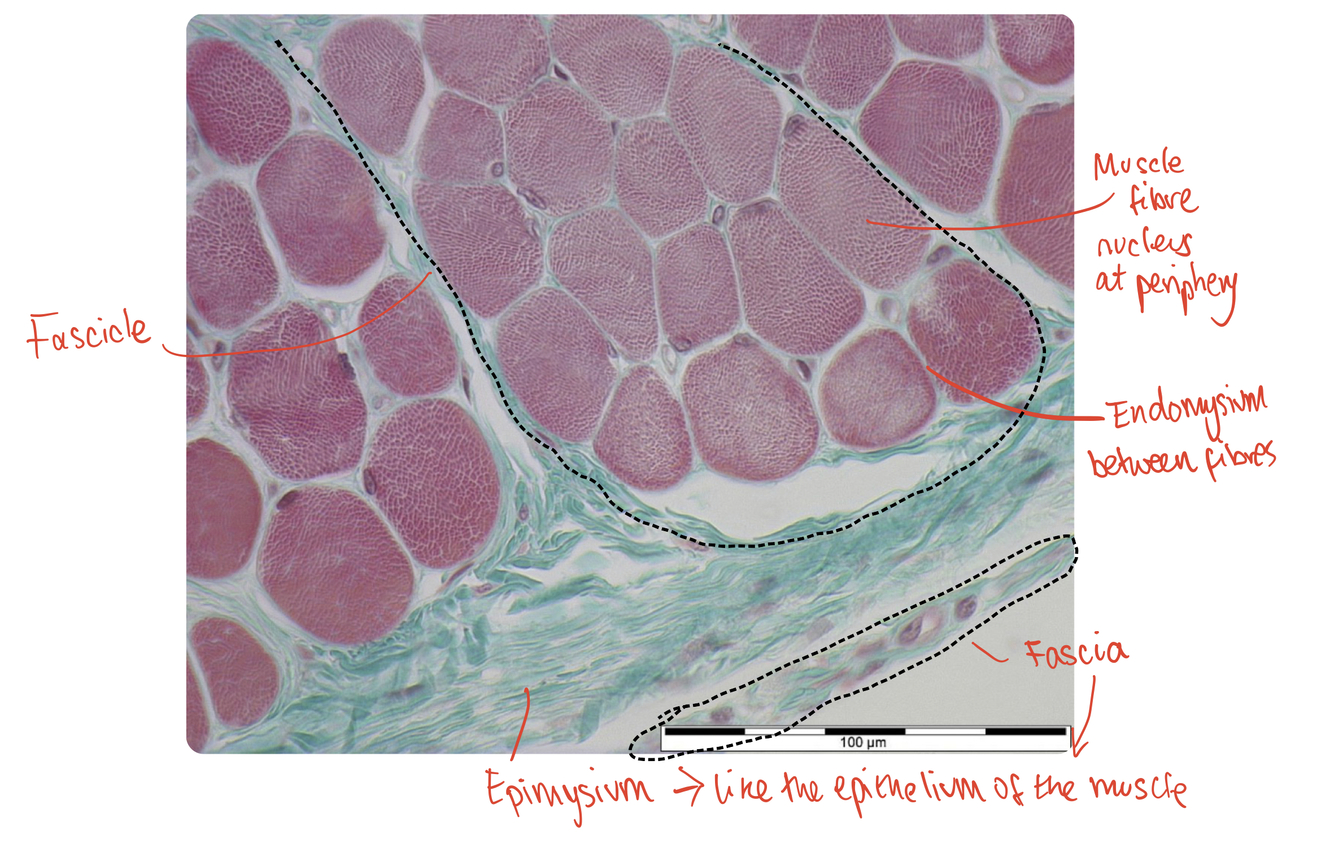
What is the endomysium ?
Connects to BM
Loose connective tissue with mixture of delicate/strong fibres that surrounds each muscle fibre
What is the perimysium ?
Mixed connective tissue , some dense, some loose, that groups muscle fibres into fascicles
where most nerves and blood vessels are found
What is the fascia ?
Dense layer of connective tissue that covers the muscle
What is the epimysium
Relatively loose connective tissue between the fascia and muscle
Identify the endomysium, a muscle fibre, the perimysium, the epimysium, a fascicle and the fascia
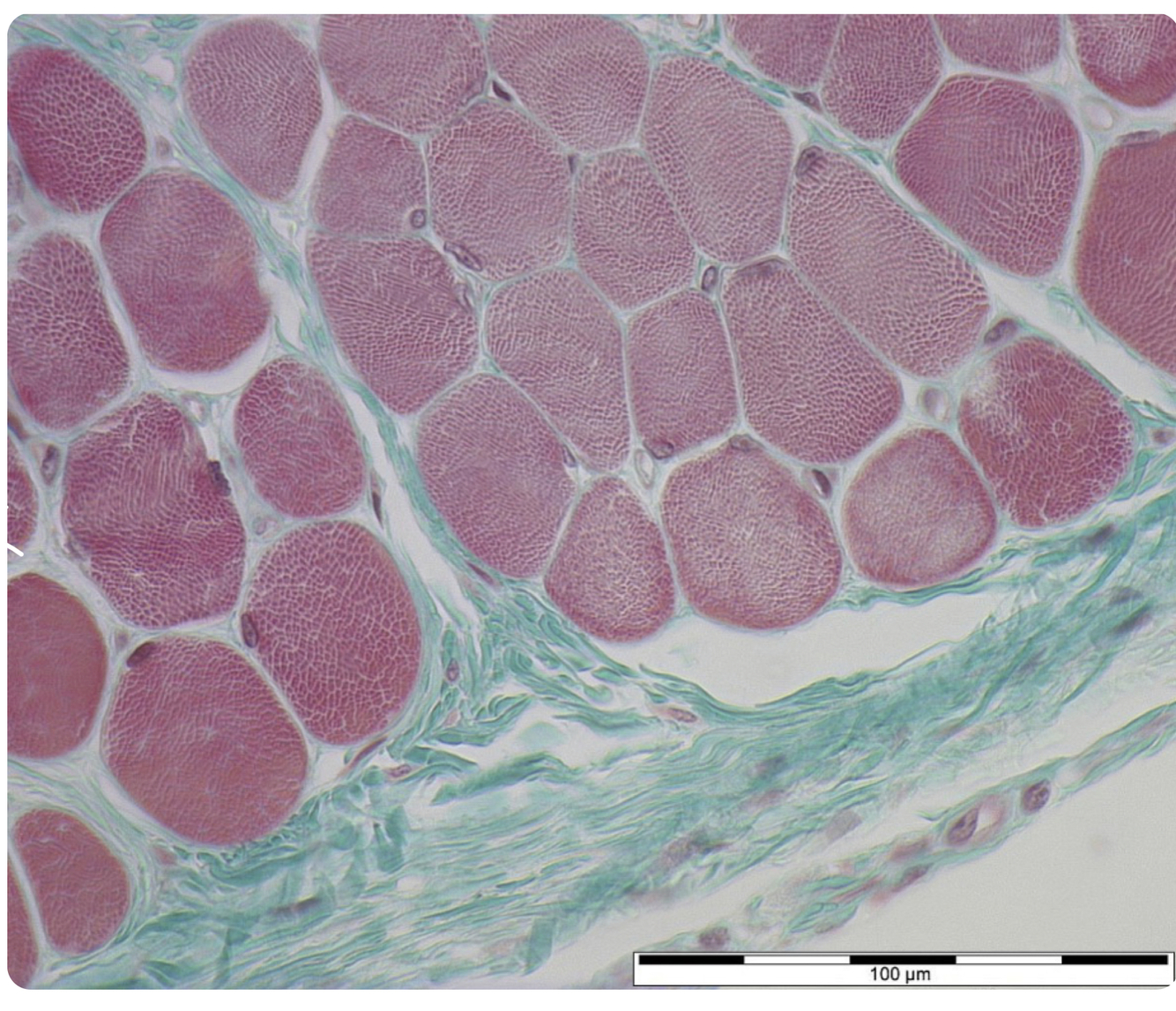
perimysium surrounds the fascicle