What anesthesia would you give to pts with MS?
- Avoid Succ!
- May have resistance OR prolonged response to NDMR
- No IV or inhaled anesthetic is superior
*
What are you monitoring for in a pt with MS?
What should you consider with emergence?
- ANS dysfunction- lower threshold for arterial line
- Consider baseline muscle weakness during emergence; extubate wide awake with full NMB reversal
Would you use regional anesthesia for a pt with MS?
- Best to avoid; may be considered in OB
- spinal anesthetics have been associated with post-op exacerbations
- because of damage to nerves, regional anesthesia may cause injury, especially if directly applied as in Spinal
- epidural anesthetics and peripheral nerve blocks have no reports of exacerbations
Guillian barre expectations during surgery
- 60% have ANS dysfunction- pt does not compensate for physiological stressors normally
- will need positive pressure ventilation d/t muscle weakness
- hypotension:
- positive pressure vent settings
- blood loss
- position change
- hypertension:
- DVL
- pain
- with indirect acting vasopressors and sympathomimetics (fluids first)
- art line mandatory
- maintain preload with fluids
- altered temperature regulation
How would you muscle relax a pt with Guillian-Barre?
- Avoid succ!
- Use a NDMR with minimal CV effects (vecuronium)
- monitor carefully for increased sensitivity or resistnace
- avoid NDMR with histamine release
What should you consider regarding extubation for a pt with Guillian Barre?
- Monitor vigilantly because they are high risk for respiratory failure!
Would you use regional anesthesia for a pt with guillian Barre?
- Epidural opioids can be beneficial for pain and discomfort
- Regional can be used with caution
- pts are sensitive to LAs (because of the Na channel blocking factor?)
- Epidural with slower onset preferred to rapid bolus of spinal
What’s the deal with Levodopa in a pt with parkinson’s?
- Remember E1/2t is short
- withdrawal effects after 6 hours
- give levodopa 20 minutes before induction and repeat prn via OG tube and post op
- If oral dose cannot be given, apomorphine SQ is a dopamine agonist that can be given
What should you consider regarding GA for a Parkinson’s pt?
- Aspiration risk- because of salivation, dysphagia, esophageal dysfunction
- RSI
- Avoid dopamine antagonists
- butyrophenones (droperidol)
- phenothiazines
- metoclopramide
- (unless you are treating L-dopa CV SE at the vasal ganglie)
- Alfentanil and fentanyl reported to cause an acute dystonic reaction
What medications can you use for your GA for a pt with Parkinsons?
inhaled agents?
NMB?
- Ketamine can be used, but can be an issue because it causes SNS/psychosis and so can dopamine
- Plan for pt to be volume depleted; have aggressive fluid plan
- Iso, Sevo, and Des acceptable
- may experience exaggerated BP decrease
- All types of muscle relaxant acceptable
Do you extubate a parkinson’s pt awake or deeply sedated?
Wide awake after full reversal criteria is met because they are likely to have respiratory complications
What drugs do you avoid during deep brain stimulation surgery?
What drugs are best?
- Avoid:
- L-dopa might be held in advance
- drugs that enhance GABA
- Best
- Opioids
- dexmedetomidine
- Avoid excessive sedation for neurologic assessment and airway management
- Communicate about any drug you are giving to the surgeon
How will you intubate a patient with a spinal cord injury?
What if they are awake and alert?
- DVL with in-line stabilization for emergency or unstable/uncertain C-spine stability
- If awake, alert, and cooperative:
- Awake fiberoptic intubation
- blind nasal intubation
- transillumination with lighted stylet
- LMA or Bullard laryngoscope
With what kind of spinal injuries would you expect more blood loss?
- Blood loss not large unless harvesting the iliac crest bone graft or vertebral body corpectomy
- Thoracic and lumbar regions have more blood loss than cervical
- expect hemodynamic instability from spinal shock
How would you expect to treat hemodynamic instability in a pt with a spinal cord injury?
- Art line required
- Elderly pts or those with significant hemodynamic lability may require PAC
- Treat with:
- aggressive fluids
- blood replacement
- continue pre-op vasopressors
- keep BP robust!
What drugs would you use for GA of a spinal cord injury?
- All inhaled and IV agents acceptable
- N2O if closed air spaces have been ruled out
- NDMR- all acceptable
- Pancuronium SNS stimulation desireable
- Succinylcholine- OK for first few hours after injury but then should be avoided forever
What are some GA concerns for a pt with a chronic spinal cord injury?
- Renal failure common
- High DVT risk
- position carefully- increased risk for fracture/skin break down
- chronic pain common
- spacsticity in skeletal muscle, often treated with baclofen
- can cause sz if interrupted
What are some medication/anesthetic agent considerations to make regarding a pt with a chronic spinal cord injury?
- Surgery may cause AD even if they have never experienced it before
- VA, epidural or intrathecal anesthesia are effective in prevention
- have vasodilator available
- No Succ! >24 hours after injury
- use NDMR
- Pts should be monitored post op for AD
- can develop after anesthetic wears off
What dose of Nitroprusside would you administer for AD?
1-2 mcg/kg
Anesthetic considerations for pts with seizures
- Consider additive effect of anticonvulsants and sedative/anesthetic drugs (both use GABA)
- Consider how anti-epileptic meds may affect organs
- coagulation, CYP450 induction
- Give anticonvulsant meds morning of surgery, intra-op, and post op
What medications must you avoid when caring for a pt with seizures?
- Methohexital
- ketamine
- etomidate
- meperidine
- atracurium and Cisatracurium (Laudanosine)
- Enflurane
- Alfentanil
How will you notice an intraoperative seizure?
What will you do?
- BP and HR changes, maybe clonic movement depending on NMB
- IV TPL, propofol or benzos
- direct application of cold saline to the surface of brain
- ABG and temp monitoring
- adjust ventilation to blow off high CO2
What are the 5 determinants of CBF?
- PaCO2
- our bes option for affecting CBF, at least for 6 hrs
- PaO2
- the hail mary
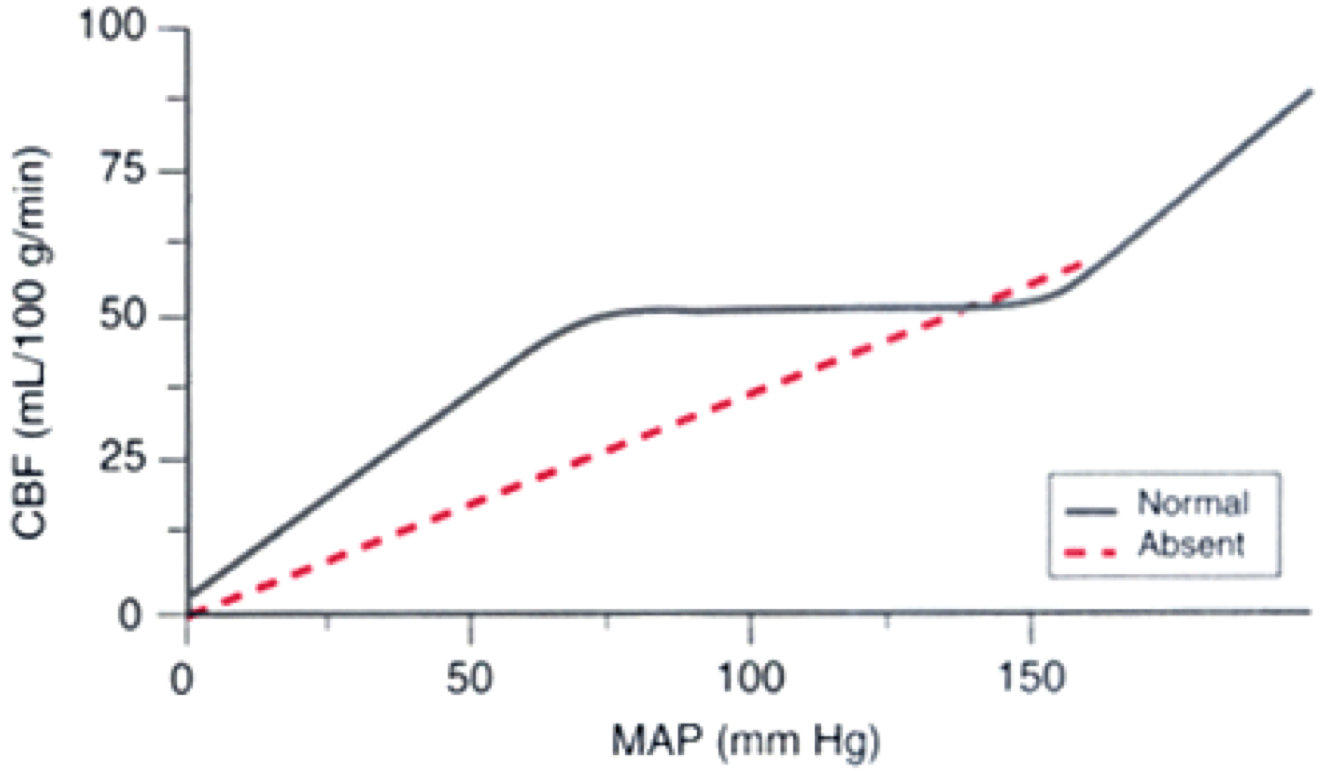
- Arterial pressure, autoregulation- btween 50-150
- Venous pressure
- head position
- Anesthetic drugs and techniques
Describe the difference in CBF between a person with normal autoregulation and one without.
(graph)

-
Induction/Emergence22
-
Anesthesia and HIV21
-
Anesthesia and other immunity diseases30
-
Cancer24
-
Musculoskeletal54
-
BIS monitoring16
-
OB59
-
Additional OB33
-
Neuro50
-
Analgesia for Labor and Vaginal delivery34
-
Pediatrics61
-
Anesthesia for C-section12
-
Renal29
-
Management of Anesthesia in a Renal pt26
-
Common Urological procedures18
-
Elderly39
-
GI26
-
Liver46
-
Pain40
-
Chronic Pain management17
-
Restrictive Lung Disease29
-
Obstructive Lung Disease24
-
Asthma31
-
Prince Caseous' special MI mini deck14
-
Frugal Casey's 1/2 price HTN deck13
-
Size isn't everything, some like 'em small- PVD16
-
Heme30
-
Heme Part 229
-
Diabetes26
-
Endocrine41
-
Obesity34
-
Obesity #219
-
Adrenal disease31
-
Adrenal #215
