Odontigenic tumours of the jaws Flashcards
(25 cards)
What is the classification?
WHO 2017 1. BENIGN A. Epithelial derived - Ameloblastoma (86%) - unicystic 13% or classical - clarifying epithelial odontigenic tumour -Adenomatoid odontigenic tumour B. Mixed derived (mes and epi) - Ameloblastic fibroma - odontoma (compound/supernumary, complex/dens) C. Mesenchymal origin - odontogenic myoxoma/myomixfibroma - cementoblastoma - cementoossifying fibroma 2. MALIGNANT - Odontogenic carcinoma (Ameloblastic carcinoma)
What is an ameloblastoma?
benign epithelial derived odontogenic tumour, second most common odontogenic tumour. -slow growing locally invasive growth from dental lamina, enamel organ and basal cells of the oral mucosa. B/L expansion. -Genes hedgehog, MAPK

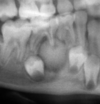
How does ameloblastoma present?
-30-40s, angle of mandible -unilocular (13%) or multilocular (classic) -soap bubble appearance with root resorption
What’s the histological presentation of Classic ameloblastomas?
-Solid tumour with islands of cystic changes
There are 6 subtypes:
- Follicular pattern- common. epithelial islands, loose stellate reticulum with columnar ameloblasts (with reverse polarity). the islands resemble enamel organ with cystic changes
- Plexiform pattern- long anastomosing chords of columnar like cells, stroma lose and vascular, cyst uncommon
- Acanthomatous 4. Granular cell 5. Basal cell 6. Desmoplastic

What is the presentation of unicystic ameloblastoma?
-younger patients (20s), posterior mandible (38/48) impacted/unerupted, asymptomatic and well circumscribed unilocular radiolecency.

What are the 3 variants of unicystic ameloblastoma?
- Luminal: confined to luminal surface of the cyst with fibrous wall of ameloblastic epithelium 2. intraluminal: 1 or more nodules of lining projections 3. Mural: follicular of flexiform infiltration. pseudomulti
How is ameloblastoma treated?
Luminal/intra: decompression/marsuplisation if large then enucleation is successful Mural/conventional: resection due to infiltrate has higher re-occurance rate BDJ Ghandi 06
What is an adenomatoid odontogenic tumour?
Benign Epithelial derived odontogenic tumour. -2-7% of odontogenic tumours. usually asymptomatic -tumour of 2/3rds. F, max canines, 20s.

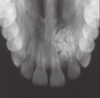
What is the radiographic appearance of an adenomatoid odontogenic tumour?
-circumscribed radiolucent unilocular lesion surrounding the crown of an unerupted tooth. -may have snowflake calcifictions

What is the histological appearance of an adenomatoid odontogenic tumour?
thick fibrous capsule -epithelial cells for rosette structure in central space -looks glandular but not -may have amyloid and calcifications
How is an adenomatoid odontogenic tumour treated?
Surgical enucleation and curettage, reoccurrence uncommon
What is a pinborg tumour (calcifying epithelial odontogenic tumour)?
uncommon 1%, asymptomatic, posterior mandible. slow growing. -PTCH mutation -30-50s.

What is the radiographic appearance of a pinborg tumour (calcifying epithelial odontogenic tumour)?
unilocular with scalloped margins -may be well defined, mixed with snow like expasions around impacted teeth
What is the histological appearance of a pinborg tumour (calcifying epithelial odontogenic tumour)?
prominent desmosomes with areas of calcification in fibrous stroma. calcifications form centric rings and then fuse to form complex masses -nuclear pleomorphism -stains green with congo red stain.
How are pinborg tumour (calcifying epithelial odontogenic tumour) treated?
enucleation and debridement of bone rim, 15% reoccurance rate
What are the two main types of mixed benign odontogenic tumours?
- ameloblastic fibroma - Odontoma
What is an Ameloblastic fibroma?
a benign mesenchymal (dental papilla) origin and epithelial origin (lamina) odontogenic tumour -20s, males, larger lesion have swelling, 70% posterior mandible. - Radio: uni or multi, well corticated on unerupted tooth -Histo: may have capsule. solid tumour of papilla like structure with epithelial chords (cub or columnar) -tx; excision and peripheral ostectomy, 18% reoccurance

What is an odontoma? (garvey)
most common mixed odontogenic benign tumour. -dental hamartoma, meaning that it is composed of normal dental tissue that has grown in an irregular way. epithelial and mesenchyme origins 2 variants: 1. Compound (supernumerary) 2. Complex (dens invaginatus)
What is a compound odontoma
more frequent, sumpernumary teeth -due to extra budding and proliferation of the dental lamina -detected in under 20s usually due to ectopic/delayed eruption . most common anterior maxilla (mesiodens) -histologically tooth structure, may be morphologically different -Tx; leave and review, removal. risk of cystic development (2, 5 yr follow ups), may cause resorption of other teeth.
What is a complex odontome?
infolding of tooth germ, does not remsemble a tooth but contains lamina and papilla remnants (epithelial and mesenchymal)
- <20, asymptomatic, molar region
- histologically appears as mature dentine and enamel clefts, epithelial ghost cells
- 20% has epithelium that has keratinised and become necrotic
- may have dentigerous cyst involvement
- Tx: excison if symptomatic

Wht are the benign mesenchymal odontogenic tumours?
- odonotogen myxoma/myxofibroma
- cementoblastoma
- cementoossifying fibroma
What is an odonotogenic myxoma?
arises from odontogenic mesenchyme
- 20-30years, posterior mandible
- B expansion when larger but asymptomatic
- scalloped margins with soup bubble appearance
- displaces and resorbs roots
- right angled trabecular
Histology: myxoid stroma containing stallate/spindle cells (hydranonic acid) may have cementum liek calcification
-tx: resection due to infiltration, not capsulated - 28%

What is a cementoblastoma?
benign mesenchymal odontogenic tumour
- young adults and children, 1%
- 75% in mandible, pain and swelling occurs
Radiographically: radioopaque mass fused to root with radiolucent halo present. Root resorption and fusion
Histological: thick sheets of trabecular mineralised with interseptal lucana and basophilic reverse line. Fibrovascular CT
- atypical giant cells
- Tx: exo with lesion
What is a cemento ossifying fibroma?
- benign fibro osseous lesion
- 30/40s, female, mandible, premolars/molars
- invades antrum, asymmetry and deformity
- radiographic: expansive well corticated unilocular mixed radiolucency somtimes also with halp
- displaced and resorbs roots, B/L expansion
Histology: capsulated well demarcated, blends into CT.
Tx: large resection, or enulceation with ostectomy. 12%
-


