Opioids Flashcards
(50 cards)
Inhibitory Neurotransmitters
gaba
glycine
Epi
NE
ACh
Endorphins
Serotonin
Histamine
Excitatory Neurotransmitters
Glutamate
Inotropic glutamate receptors - NMDA
Glutamate
- located in the hippocampus, cortex, and substantia gelatinosa
- learning, memory, recall
- central pain transduction
- excitotoxic neuronal injury
Opioids
- most efficacious analgesic drug available
- agonists on mu, kappa, delta receptors
- may not totally eliminate pain
Opioid activation of mu receptor
- produce analgesia
Opioids _______ Ca++ influx and _____ K+ efflux.
Opioids block Ca++ influx and increase K+ efflux.
Opioid MOA on receptors
- agonist at stereospecific opioid receptors in pre- and post- synaptic sites in CNS and peripheral nerves
- activate opioid receptors on primary afferent sensory neurons (also activated by enkephalins, endorphins, dynorphins)
- need to be ionized for strong bonding to receptors
Levo-rotary opioid molecules
- only levo-rotary opioid molecules exhibit agonist activity (so anything besides levo-rotary won’t give us pain relief!)
Opioid MOA 2 - neurotransmission
- Principal effect of opioid receptor activation is by decreased neurotransmission!
- occurs by presynaptic inhibition of release of NTs (ACH, dopamine, NE, substance P)
Opioid receptor occupied by agonist
- increased K+ conductance hyperpolarizes membrane
- and/or Ca+ ch inactivation
- leads to decreased NT release and decreased transmission of pain!
Opioid action on peripheral nerves
Opioids do NOT alter the responsiveness of peripheral nerves to noxious stimuli nor do they impair impulse transmission
Opioids cross the BBB based on 4 things:
- Molecular size (smaller = better)
- lipid solubility (more lipid sol = better)
- non-ionized is better (more lipid soluble)
- protein binding (greater protein binding = less drug available to cross BBB)
Lipid Solubility and Protein Binding Chart

Morphine Lipid Solubility and Protein binding
23% nonionized at pH 7.4 (able to cross BBB)
1.4 lipid solubility (slow onset of action)
35% protein binding (65% available for action)
Fentanyl Lipid Solubility and Protein binding
9% nonionized at pH 7.4
816 lipid solubility
84% protein binding
Alfentanyl Lipid Solubility and Protein binding
89% nonionized at pH 7.4
128 lipid sol
92% protein binding
Remifentanyl Lipid Solubility and Protein binding
58% nonionized at pH 7.4
18 lipid solubility
70% protein binding
Opioid Receptors and Endogenous Opioids

Mu Receptors Location and Actions

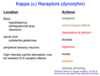
Kappa Receptors (dynorphin) Location and Actions
Delta Receptors Location and Action

Nagelhout and Plaus Table 12-2

Generalizs opioid SE - Resp, GI, CV
- sedation (precursor to respiratory depression)
- resp dep (prevented by intense pain)
- N/V (give antiemetics)
- decreased GI motility (give stool softener)
- CV effects: orthostatic hypotension, bradycardia, and peripheral vasodilation (2/2 histamine release)
Generalized opioid SE 2
- euphoria (meperidine)
- antitussive (codeine)
- miosis (pupillary constriction)
- pruritis
- biliary spasm (gallbladder surg)
- myoclonus/sz’s
- chest wall rigidity (high doses may cause difficult mast ventilation, give muscle relaxer)


