Mx of Phobia
Desensitisation or CBT
Consider specific interventions e.g. community dental officer in phobia of dentists
Rx not routinely used
DDx in GAD?
What differentiates GAD from these
• Depression: Anxiety symptoms are common in depression and co-morbid
depression is often seen with GAD. The type of symptom that appears first and is
more severe is conventionally considered to be primary.
• Panic disorder: There is a discrete episode of intense fear with sudden onset and a
subjective need to escape.
• Other anxiety disorders: They have the same core symptoms as in GAD but the
symptoms occur in specific situations as in phobic anxiety disorder, OCD or PTSD.
• Substance misuse: Symptoms of alcohol or drug withdrawal may mimic those of
anxiety.
• Physical illness: A host of medical conditions can mimic GAD – endocrine disorders
such as hyperthyroidism or phaeochromocytoma; neurological disorders such as
migraine; deficiency states such as anaemia or vitamin B12 deficiency; cardiac
conditions such as arrythmias and mitral valve prolapse, and metabolic conditions
such as hypoglycaemia and porphyria.
GAD is not situation dependent
Autonomic symptoms may be present
Stepped care model in GAD
Identify, asess, educate, monitor
No improvement: low-intensity psychological support e.g. primary care counselling
GAD with inadequate response to step 2 or marked functional impairment:
CBT (first line) or drug treatment (SSRIs e.g. sertraline first line although unlicensed, then paroxetine or escitalopram)
If GAD remains refractory:
Specialist drug and or psychological treatment, crisis intervention, outpatient or inpatient care
Mx of OCD in adults
Mild functional impairment:
Referral to IAPt for low-intensity psychological therapies (CBT + Exposure response prevention, group CBT couples based course)
SSRI may be useful
Moderate functional impairment:
High intesnity CBT + ERP or SSRI (clomipramine may also be used as an SSRI alternative)
Severe functional impariemtn:
High intensity CBT +ERP AND SSRI
Mx of OCD in children
Mild dysfunnction:
Guided self-help or refer to CAMHS
Moderate to severe:
Refer to CAHMS: CBT and ERP but will involve family
If psychological treatment fails:
Investigae other factors that are affecting
In children >8 SSRi might be appropriate but should only be prescribed following paediatric psychiatrist specialist assessment of child
Stepped care approach to panic attacks
Treat in primary care: involve family, avoid anxiety-producing substances e.g. caffiene. Exclude DOA
CBT first line
Medication: SSRI unless CIed
Consider imipramine or clomipramine if this fails
Self help
If two interventions have been offered without benefit, consider referral to specialist mental health services
No Benzos
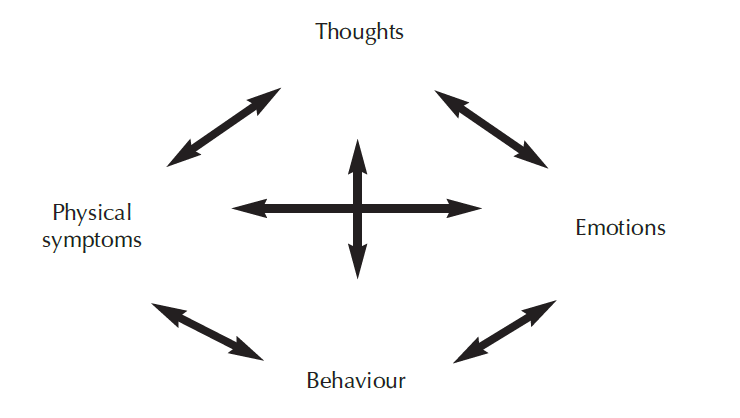
Draw the hot cross bun model in CBT
NICE guidleines when depression and anxiety co-exist
Treat depression first
Mx of depression
Mild
Moderate to severe
Severe
CBT or low-intensity psychological therapy first line
Moderate-to severe: CBT and SSRI
What are the indications for referral in depression?
Uncertain diagnosis, including possible bipolar disorder.
Failed response to two or more interventions.
Recurrence of depression <1 year from previous episode.
More persistent suicidal thoughts.
Comorbid substance, physical, or sexual abuse.
Severe psychosocial problems.
Rapid deterioration.
Cognitive impairment.
What is important in every case of anxiety disorder?
Ask questions about depression and risk
What are the key components of motivational interviewing techniques?
Shown to be more effective in dealing with substance misuse
- Use of empathy to understand patients point of view
- Allow the patient to explore the discrepancy between positive core values and his unhealthy behaviours
- Tackling the inevitable resistance with empathy rather than confrontiation
- Supporting self-efficacy and enhancing self-esteem
What is the step-wise treatment to opioid use
Based on principle of harm minimisation:
- reduce injecting
- reduce street drug use
- mainteance thrapy with heroin substutes (methdone or buprenorphine)
- reduction in substitute prescribing
- abstinence
What can be used as mood stabilising prophylaxis in women of child-bearing age?
Olanzapine
Biopsychosocial management of BPAD
Social:
Care programme appraoch
Involve friends/relatives
Advance directive
Serious mental illness register
Psychological:
Self-help
CBT: helps with trigger avoidance
Biological:
Depends on stage in cycle
Ddx for stridor in an infant
Laryngomalacia
Laryngeal cyst, haemangioma or web
Laryngeal stenosis
Vocal cord paralysis
GORD
Vascular ring
Hypocalcaemia (laryngeal tetany)
Respiratory papillomatosis
Subglottic stenosis
What differentiates between stridor and wheeze
Stridor is predominantly inspiratory
Wheeze expiratory
Mx of croup
Oral dexamethasone (nebulised budesonide may also be used)
If has improved 2-3h later and SaO2 >95-> discharge
If not, further dose of steroids can be administered 12-24h later.
If the child deteriorates further then nebulised adrenaline can be administered. Senior help and anaesthetics should be summoned
Intubation and ventilation are necessary if there is still no control
What are the indications for hospital referral in bronchiolitis
Poor feeding (<50% usual intake over the previous 24 hours) which is inadequate to maintain hydration
Lethargy
History of apnoea
Respiratory rate >70 breaths/minute
Nasal flaring or grunting
Severe chest wall recession
Cyanosis
Saturations ≤94%
Uncertainty regarding diagnosis
Where home care or rapid review cannot be assured
Secondary care mx of bronchiolitis
Supportive
CXR only indicated if unusual clinical course
Blood tests only if there is diagnositc uncertainty e.g. >39 temperature
Keep SaO2 >92
NG fed if they cannot maintain >50% of normal intake
CBG if there is deterioriation
CPAP may be used as an alternative to intubation
Ddx of a recurrent or persistent cough in childhood
Recurrent viral URTIs – very common in all age groups but more so in infants
and toddlers
• Asthma – unlikely without wheeze or dyspnoea
• Allergic rhinitis – often nocturnal due to ‘post-nasal drip’
• Chronic non-specific cough – probably post-viral with increased cough receptor
sensitivity
• Post-infectious – a ‘pertussis (whooping cough)-like’ illness can continue for
months following pertussis, adenovirus, mycoplasma and chlamydia
• Recurrent aspiration – gastro-oesophageal reflux
• Environmental – especially smoking, active or passive
• Suppurative lung disease – cystic fibrosis or primary ciliary dyskinesia
• Tuberculosis
• Habit
Signs of impending respiratory failure
Exhaustion (this is a clinical impression)
• Unable to speak or complete sentences
• Colour – cyanosis pallor
• Hypoxia despite high-flow humidified oxygen
• Restlessness and agitation are signs of hypoxia, especially in small children
• Silent chest – so little air entry that no wheeze is audible
• Tachycardia
• Drowsiness
• Peak expiratory flow rate (PEFR) persistently 30 per cent of predicted for height
(tables are available) or personal best. Children 7 years cannot perform PEFR
reliably and technique in sick children is often poor
What is an important consideration in giving continuous nebulised salbutamol
Cardiac monitoring is indicated as this can lead to side effects
What are the components of an asthma review?
How often does he miss his regular drugs?
• Is there parental supervision?
• What device does he use? Children rarely use MDIs effectively and need a spacer.
However, he is unlikely to use one because they are cumbersome and not ‘cool’.
Agree an alternative ‘breath-activated’ device with the proviso that, if acutely
wheezy, he must use a spacer.
• Consider changing to a combined steroid/long-acting β-agonist inhaler. This should
improve adherence.
• Ask about smoking – him and his family. Adults should be encouraged to stop
smoking or to smoke outside.
• Educate about allergen avoidance, e.g. daily vacuuming to reduce house dust mites.
Consider measuring total IgE and specific allergen IgE (RAST) if the history suggests
allergies.
• All asthmatics should have a written home management plan.
Provide an asthma symptom diary and arrange hospital follow-up until control
improves. Most children can and should be managed in primary care. Primary care
and hospital-based asthma specialist nurses are very helpful.




-
Hypopituitarism33
-
Hypersecretion of anterior pituitary hormones21
-
Neurohypophyseal disorders25
-
Hypothyroidism15
-
Hyperthyroidism35
-
Psychiatry209
-
Paediatrics409
-
Gynaecology202
-
Obstetrics326
-
Histopathology408
-
Microbiology463
-
Haematology301
-
ChemPath321
-
Immunology270
-
Psych704
-
O&G1793
-
Paeds1990
-
PACES177
-
Eponymous Syndromes / Diseases4
-
Micro Buzzwords78
-
Haematology COPY51
-
O&G COPY39
-
Paeds COPY58
-
Psych COPY22
-
Immuno63
-
Eponymous Psych Syndromes13
-
Chem path6
