Asthma - def? Presentation? Ix? Severity? Short-term/long-term Mx incl. conservative? Mneumonic for conservative long-term Mx?
Def: chronic inflammatory airway disease characterized by reversible airway obstruction + airway hyperresponsiveness
Presentation
- Dry cough, polyphonic wheeze ( worse@night/morning)
- Triggers: cold air, pollen, pollution, exercise
- Atopic features - eczema, nasal polyps
Ix:
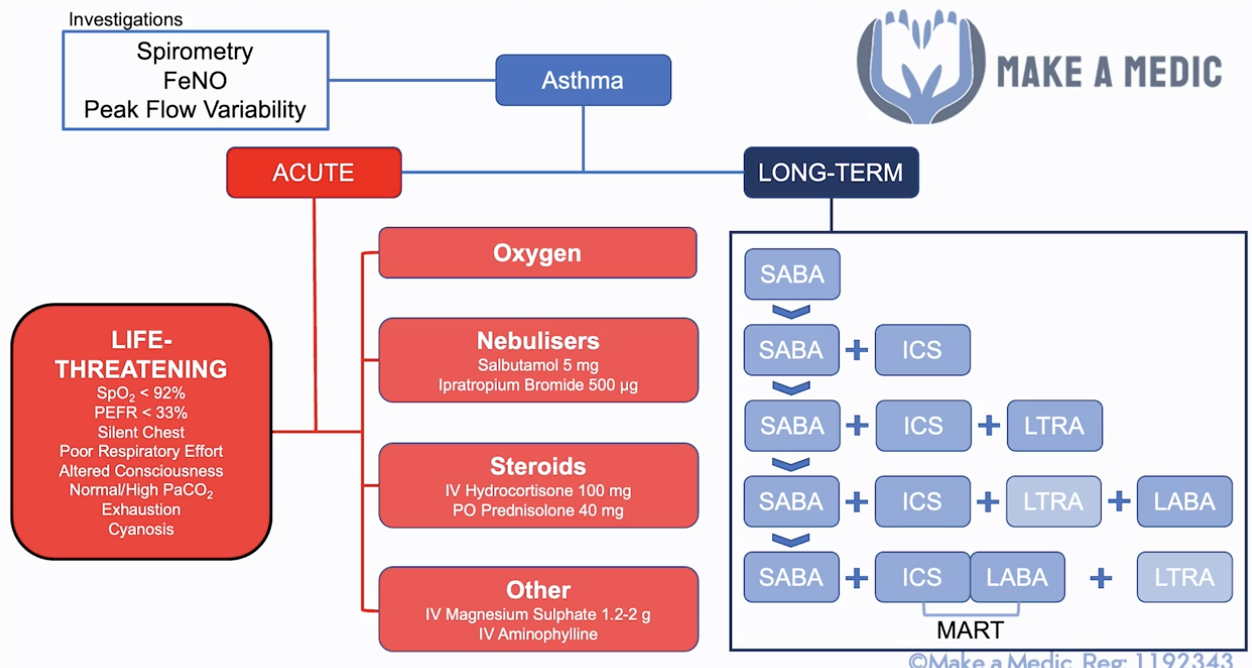
- Peak flow variability (in peak flow diary)
- Spirometry (shows reversibility after bronchodilator)
- FeNO (fractional exhaled nitric oxide - a marker of airway inflamme, in uncertain Dx)
- On exacerbation:
- ABG, peak flows (min x4/day), CXR
- Other:
- Allergy testing - total IgE, specific IgE (RAST), serum eosinophil count
Asthma severity:
- Life-threatening: PEF <33% of baseline/SpO2 <92%/PaO2 <8/Normal or raised PaCO2 - should be low with resp alkalosis due to excess breathing only becomes acidotic when get tired
- CHEST: Cyanosis, Hypotension, Exhaustion, Silent chest, Tachycardia
- Acute severe: PEF <50% of baseline/RR >25/HR >110/can’t complete sentence without taking a breath
- Moderate: PEF <75% of baseline
Short-term Mx:
- A-E approach, seek senior support (call for help if life-threatening)
- O2 - 15L NRM (if hypoxaemic)
- Burst therapy:
- SABA (spacer up to 10 puffs every 20 mins –> nebs)
- Ipratropium Bromide (add to nebs if poor response/severe, every 4-6hrs)
- Corticosteroids (min 5-day course, give within 1 hour, give IV if can’t take orally)
- Other Tx options:
- IV Magnesium sulfate (STAT dose if poor response above/severe) - consult senior before use
- IV salbutamol (if on ventilation) - consult senior before use
- IV Aminophylline - consult senior before use, requires ITU setting
- If less distressed/more tired/shallow breaths/confused –> call critical care outreach team (CCOT) for ITU support
Long-term Mx (>16yrs):
- Conservative: TAME
- Technique
- Avoid triggers
- Monitor peak flow
- Educate - formulate Personalised Asthma Action Plan (PAAP), Annual flu vaccine
- Medical:
- SABA (reliever)
- SABA + ICS (preventer)
- SABA + ICS + LTRA (leukotrine receptor antagonist e.g. montelukast)
- SABA + ICS + LABA (+ LTRA stopped unless good response)
- SABA + MART (ICS + LABA COMBO) (+ LTRA)
- NOTE: maintenance & reliever therapy (MART) - used as preventer & maintenance inhaler
- Specialist input (e.g. for oral steroids)
COPD - definition? Signs & Sx? New Dx & exacerbation Ix/Mx? Prognosis factors?
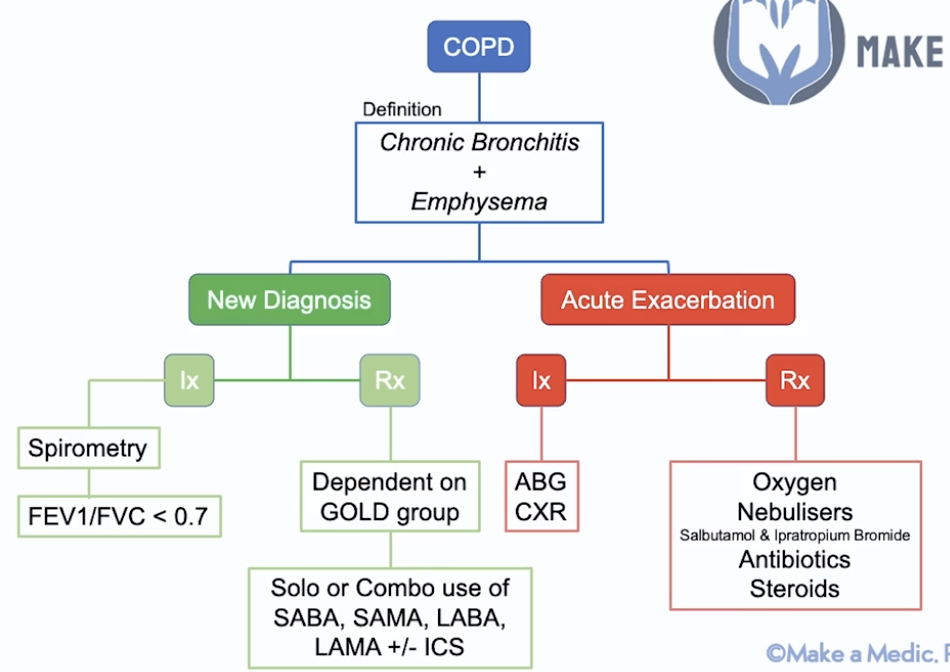
Def: chronic bronchitis (damaged to cilia in bronchi - blue bloater) + emphysema (damage to alveoli - pink puffer)
Presentation:
- Cough (productive), SoB (starts on exercise)
- RF exposure - smoking/pollution
- Signs:
- Barrel chest
- Hyper-resonant (air trapping)
- Reduced breath sounds
- Widespread expiratory wheeze
- Coarse crackles if exacerbation (mucus in airways)
- Other - asterixis (CO2 retention flap), raised JVP (cor pulmonale)
- NOTE: COPD does not cause clubbing –> cancer/bronchiectasis
New Dx Mx:
- Ix:
- Bedside - mMRC dyspnoea scale, O2 sats, ECG (cor pulmonale)
- Spirometry - FEV1/FVC <0.7 (forced exp volume in 1s)
- Mild - FEV1 ≥ 80%
- Moderate - FEV1 ≥ 50%
- Severe - FEV1 ≥ 30%
- Very severe - FEV1 <30%
- Bloods - FBC, ABG, eosinophil count, alpha1-antitrypsin level
- Imaging - CXR, CT chest
- Other: serial peak flows if asthma DDx, sputum culture (in freq exacerbation), pul funct tests
- Mx:
- Conservative - stop smoking, influenza + pneumococcal vaccine, inhaler device training
- Persuade to stop smoking
- Pul rehab
- Prick them - influenza + pneumococcal vaccine
- Psych issues
- Medical - depends on severity - GOLD group –> solo/combo of:
- SABA e.g. salbutamol
- SAMA e.g. Ipratropium bromide
- LABA e.g. salmeterol
- LAMA e.g. tiotropium
- ± ICS e.g. beclomethasone
- Other: mucolytic e.g. acetylcysteine, O2 therapy, theophylline
- Medical pathway:
- 1 - SABA/SAMA
- 2a - Steroid-responsive (eosinophilia/atopy): LABA + ICS
- 2b - Not steroid-responsive: LABA + LAMA
- 3 - LABA + LAMA + ICS
- 4 - specialist input e.g. theophylline
- Surgical - lung reduction surgery (large bullae)
- Other: long-term O2 therapy
- Only if non-smoker (smoker –> burns)
- Only if <7.3 PaO2/<8 if also pul HTN
- Only if PaCO2 does not rise excessively on O2
- Conservative - stop smoking, influenza + pneumococcal vaccine, inhaler device training
Acute Exacerbation Mx:
- Ix: ABG, ECG, CXR
- Mx:
- 15L O2 NRM
- Nebs - salbutamol + IpB
- Steroids (PO pred/IV hydrocortisone)
- Abx if infective –> prophylactic abx if persistent infections - azithromycin
Prognosis factors:
- Body mass - worse if obese
- Obstruction - worse if reduced FEV1
- Dyspnoea
- Exercise capacity - how far can you walk in 6 minutes?
Complication –> vasoconstriction to redirect blood flow to well-oxygenated areas of the lungs –> if widespread –> pul HTN –> cor pulmonale
Pneumonia - def? Presentation? Types? Ix? Scoring? Mx?
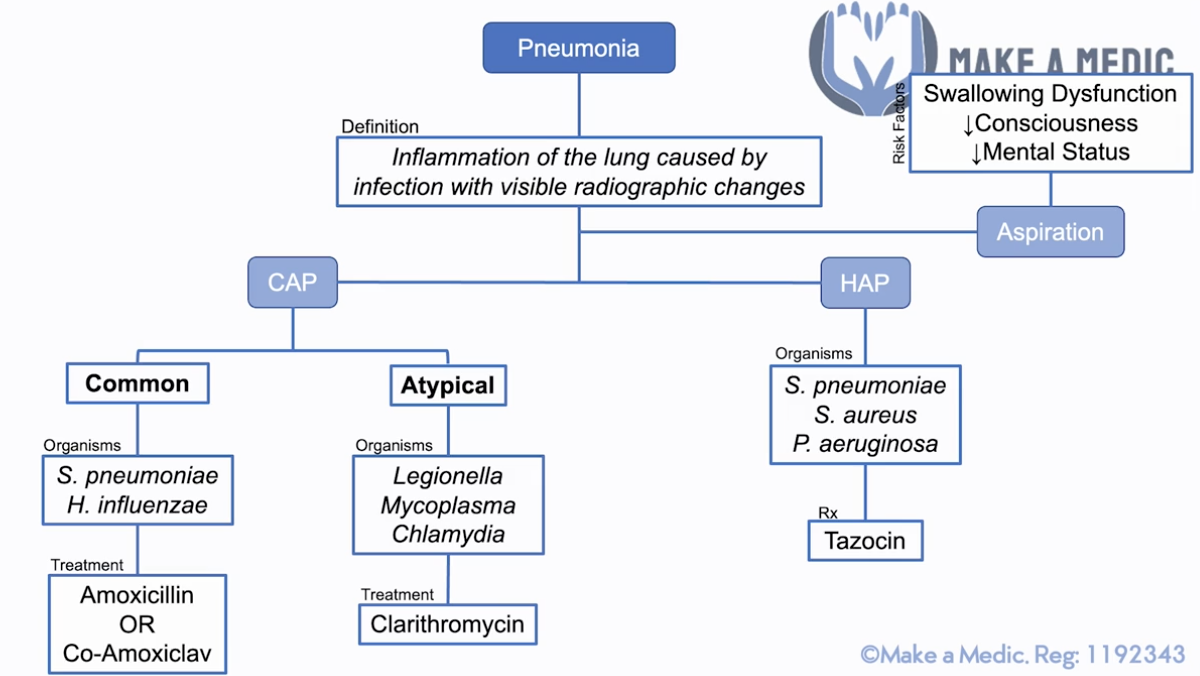
Def: inflammation of lung caused by inf w/ visible radiographic changes
Presentation:
- Decreased chest expansion, dull on percussion, increased sound vocal resonance
- Coarse crackles
- Bronchial breathing – bronchial airflow instead of alveolar airflow (due to transmission of sounds through consolidation) – check by listening to sound at the throat
Ix: ABG, CXR, sputum culture (mod/high severity)
Scoring for CAP: CURB-65 (confusion, urea ≥7mmol/L, RR ≥30, BP <90/60, ≥65yrs)
- +1 = outpatient; +2 = outpatient/inpatient, +3 = inpatient ± ITU
- NOTE: urea is no longer used
Types & Mx –> local abx guidelines
- CAP:
- Typical (S. pneumo, H. influenzae) –> Amox/Co-Amox
- Atypical (Legionella, Mycoplasma, Chlamydia) –> Clari
- Dry cough (instead of productive), myalgia, confusion, diarrhoea
- NOTE: if not sure often given Co-Amox + Clari
- HAP - pneumonia arising >48hrs after admission to hospital (S. pneumo, S. aureus, P. aeruginosa) –> Taxocin (pseudomonal cover)
- Aspiration - RFs: swallowing dyfunct, reduced consciousness, reduced mental status –> elderly/frail
Goes into septic shock –> give IV fluid + senior help + check abx sensitivity (ring lab) –> ITU (intropic support - NA to increase PVR)
- Other aspects of septic-6
- NOTE: dobutamine is for cardiogenic shock to increase CO - this is not relevant here
PE - def? Sx? RFs? Scoring & Ix? Mx?
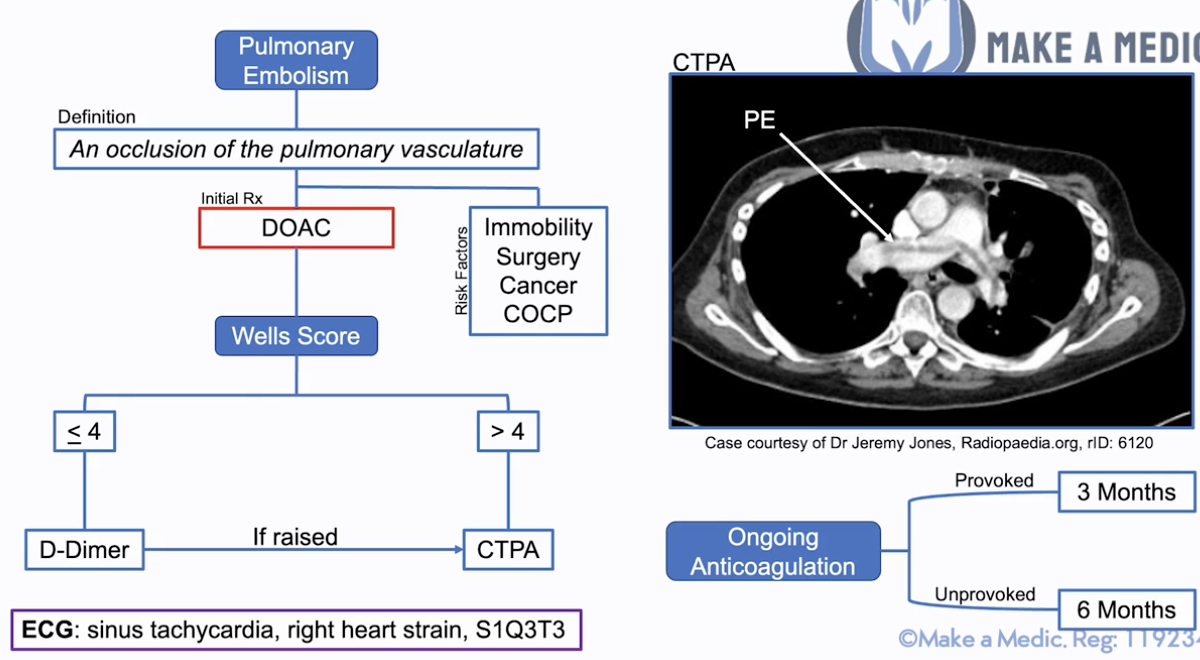
Def: occlusion of pulmonary vasculature characterized by sharp pleuritic chest pain
Sx: SYNCOPE, sudden SoB, pleuritic chest pain, haemoptysis
RFs: SICC - Surgery, Immobility, Cancer, COCP
Initial Tx:
- DOAC (e.g. Apixaban) or unfractionated heparin (if bleeding risk, can be reversed easily)
- Massive PE –> IV unfractionated heparin for hours before and after thrombolysis e.g. IV alteplase
Scoring & Ix: Well’s score
- ≤4 = D-Dimer –sign raised–> CTPA
- >4 = CTPA
- ECG useful - sinus tachycardia, right heart strain, S1Q3T3
- NOTE: Troponin = useful markers for PE severity (indicates right heart strain)
Ongoing anticoagulation - DOAC/Warfarin
- Provoked - 3 months (SICC)
- Unprovoked - >6 months + cancer & thrombophilia testing
- Ix for cancer –> any Sx?
- If yes - CT TAP
- If no - FBC, U&E, LFTs, clotting, physical exam –> if concern –> CT TAP
- Consider thrombophilia screen if no cancer for anti-phospholipid syndrome (anticardiolipin, lupus anticoagulant, anti-beta-2-glycoprotein)
- Ix for cancer –> any Sx?
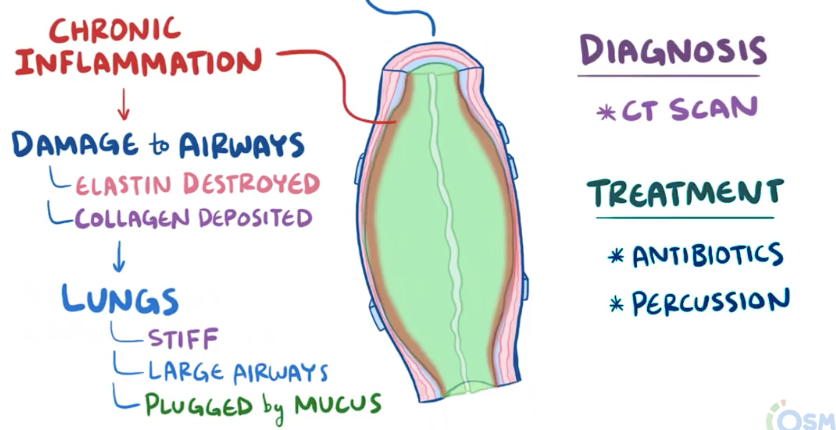
Bronchiectasis - definition? causes? presentation? Ix? Mx?
Def: obstructive lung disease characterised by permanent dilation of bronchi from the destruction of elastic & muscular components of the bronchial wall
- Results from diseases causing chronic inflammation:
- Primary ciliary dyskinesia - cilia don’t move –> mucus trapped in airways –> recurrent pneumonia –> chr inflammation
- Cystic fibrosis - mucus thick & sticky –> recurrent pneumonia –> chr inflammation
- Airway obstruction - tumour inside/outside airway or inhaled foreign body –> mucus can’t clear –> recurrent pneumonia –> chr inflammation
- NOTE: worse with certain infections e.g. aspergillosis –> hypersensitivity response
- Chr inflammation - has immune cells that release cytokines –> damage ciliated epithelial cells + destroys elastin –> airways dilated + clogged with mucus –> fibroblasts deposit collagen –> stiff lungs + mucus plug –> obstructive lung disease
Presentation:
- RFs: CF, PCD, congenital disorders of airway, host immunodef (incl. HIV), recurrent lung inf
- Less common - inhaled foreign body, connective tissue disease, IBD, alpha1-antitrypsin def
- Productive cough (large amounts of sputum) ± haemoptysis - worse lying flat/one side
- Dyspnoea (with increased severity)
- Fever (on exacerbation)
- Crackles, inspiratory squeaks & rhonchi, clubbing (from long-term hypoxia)
Ix: CXR (ring shadows, tramlines), high-res CT (signet ring sign), FBC + sputum culture & sensitivity (inf e.g. pseudomonas), pul function tests
- Genetic testing (for possible RF causes): serum alpha1-antitrypsin, serum Ig lvls (ID), specific IgE for Aspergillus, sweat Cl test (CF), rheumatoid factor (CTD), HIV test, nasal nitric oxide (PCD)
Mx:
- Conservative:
- Persuade to stop smoking
- Pul rehab
- Prick them - influenza + pneumococcal vaccine
- Psych issues
- Medical:
- Mucoactive agent (nebulised hypertonic saline)
- Inhaled bronchodilator (SABA/SAMA/LABA/LAMA) - ONLY If co-existing asthma/COPD
- Surgical: depending on primary cause e.g. IFB, tumour –> lobectomy/lung transplant
- Exacerbation: short-term abx (azithromycin)
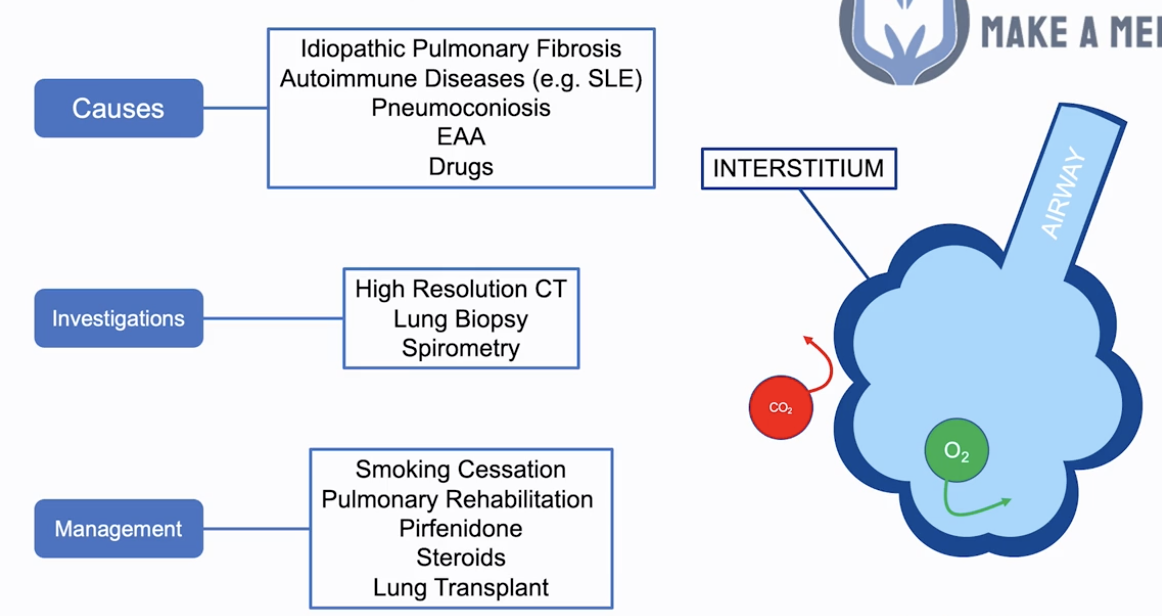
Interstitial lung disease - causes? presentation? Ix? Mx? Prognosis?
Interstitial lung disease
- Refers to the tissue the gasses pass through e.g. surface of alveoli –> reducing gas exchange
Causes:
- Upper zone fibrosis: PATEN (more occupational causes)
- Pneumoconiosis (not asbestosis) - caused by inorganic dust (e.g. soot)
- Aspergillosis/ABPA
- TB
- Extrinsic allergic alveolitis - caused by organic dust e.g. animal shedding
- Negative seroarthropathies
- Lower zone fibrosis: STAIR
- Sarcoidosis
- Toxins: B-MANS (Bleomycin, Methotrexate, Amiodarone, Nitrofurantoin, Sulfasalazine)
- Asbestosis
- Idiopathic pulmonary fibrosis
- Rheum: SLE, RhA etc
- Signs of conditions associated w/ pulmonary fibrosis:
- MCP swelling - RA
- Malar rash - SLE
- Kyphosis - Ank Spond (apical fibrosis)
- Lupus pernio - sarcoidosis
- Thick skin/’bird beak’ nose - systemic sclerosis
- Aphthous ulcers, abdo scars - Crohn’s
- Grey skin - amiodarone
Main Sx: progressive SOBOE, dry cough, fatigue, weight loss
Signs: find end-insp creps, clubbing
- Other: reduced chest expansion, normal/reduced percussion, normal vocal fremitus
Investigations: spirometry, high-res CT & lung biopsy
- Bedside: spirometry (low FEV1, low FVC, FEV1/FVC>0.8 = restrictive lung disease), ECG (right heart strain), drug review
- Bloods
- FBC, U&E, LFTs, CRP, ESR, ABG (T1RF)
- AI screen - Serology (CTD): ANA, RhF, anti-CCP
- Serum ACE for sarcoidosis
- TB testing
- Imaging
- CXR: reticulonodular shadowing (honeycombing) + rule out lung cancer
- High-res CT: more detailed view of alveolar structure –> ‘honeycombing’ + lung biopsy
- Echo (right heart strain/cor pulmonale)
- Invasive
- Bronchoscopy + lung biopsy (gold-standard)
Management:
- Conservative (4Ps):
- Persuade to stop smoking, reduce exposure (meds, EAA)
- Pul rehab
- Prick them - influenza + pneumococcal vaccine
- Psych issues
- Medical: anti-fibrotic e.g. pirfenidone +/- prednisolone ± O2 (if hypoxaemic)
- Surgical: lung transplant if severe deterioration/impairment/oxygen dependent
Prognosis: 3-4yrs post-Dx (no Mx increases survival)
Pleural effusion - signs? causes? Ix? Mx?
Signs (if fluid > 300ml):
- Key:
- Stony dull in lung base
- If large: tracheal deviation away
- Reduced chest expansion
- Reduced breath sounds
- Reduced vocal fremitus
Causes:
- Transudative (<30g/L protein)
- HEART FAILURE
- Hypoalbuminaemia: liver disease, nephrotic syndrome, malabsorption
- Hypothyroidism
- Meig’s syndrome (benign ovarian tumor + ascites + pleural effusion)
- Exudative (>30g/L protein)
- Infection: PNEUMONIA, TB, subphrenic abscess
- Connective tissue disease; RA (also low glucose), SLE
- Neoplasia: lung cancer, mesothelioma, metastases
- Pancreatitis: high amylase in pleural fluid
- Pulmonary embolism
Ix:
- Bedside: obs, urinalysis for protein
- Bloods:
- ABG, BC
- FBC, U&E, LFTs, CRP
- Clotting (before needle aspiration), albumin (nephrotic syndrome)
- Mantoux/ELISPOT (TB)
- Imaging:
- CXR: meniscus sign, dense shadowing, pleural effusion if ≥300mL fluid
- CT chest - identify the cause
Management: US-guided pleural aspiration = thoracocentesis (21G needle, 50ml syringe) - above rib to avoid NV bundle
- LDH & protein in pleural fluid & serum + RBCs, WBCs, cytology, culture, pH & glucose of pleural fluid
- MC&S
- Biochemistry: PPALS
- Protein (also serum)
- pH
- Amylase
- LDH (also serum)
- Sugar (glucose)
- Cytology
- Immunology - if indicated (RF, ANA, complement)
- Findings:
- Protein > 30g/L: exudate
- Protein < 30g/L: transudate
- Protein 25-35g/L: use Light’s criteria. An exudate is likely if at least 1 of:
- Pleural protein/serum protein > 0.5
- Pleural LDH/serum LDH > 0.6
- Pleural LDH > 2/3 upper limits of normal serum LDH
- Tx cause e.g. abx for infection, furosemide for HF
- Management of recurrent pleural effusion
- Recurrent aspiration (thoracocentesis)
- Pleurodesis
- Indwelling pleural catheter
Pleural fluid features:
- Heavy blood staining - mesothelioma, TB, PE, trauma
- Purulent/turbid/cloudy - empyema secondary to bacterial pneumonia –> insert chest tube to allow drainage
- Milky - chylothorax via lymphatic obstruction secondary to malignancy
Pneumothorax - Def? RFs? Causes? Ix? Mx? How do you identify a Tension Pneumothorax?
Pneumothorax = accumulation of air in pleural space (subdivided into primary and secondary)
RFs: pre-existing lung disease, Marfan’s, RA, smoking
Causes: cystic pathology, parenchymal necrosis, iatrogenic, trauma
Ix: CXR
Mx:
- Primary (no pre-existing lung disease)
- <2cm (betw lung margin & chest wall), no SoB – observe 4-6hrs ± supplemental O2
- SoB/≥2cm – needle aspiration (16-18G) –> observe 4-6hrs
- Do NOT repeat needle aspiration x2
- Chest drain if above fails + ADMIT ± supplemental O2
- NOTE: correct clotting before inserting if possible
- Surgery
- Secondary (pre-existing lung disease) - ADMIT all secondary pneumothorax (for at least 24hrs observation)
- <1cm - high-flow O2 + ADMIT (24hrs observation)
- 1-2cm - needle aspiration (16-18G) –> high-flow O2 + ADMIT (24hrs observation)
- SoB/≥2cm/previous failed - chest drain + ADMIT ± supplemental O2
- Surgery
Tension pneumothorax = pushes away the trachea to the opposite side
- Non-traumatic:
- IMMEDIATE peri-arrest call (2222)
- Needle decompression = emergency Tx, 2nd ICS MCL (grey cannula) + high-flow O2
- Follow-up = ADMIT + chest drain
- Traumatic:
- Open thoracostomy
- Follow-up = ADMIT + chest drain
- Traumatic non-tension pneumothorax:
- High-flow O2 + ADMIT (24hrs observation)
- If open pneumothorax/penetrating chest wound –> occlusive dressing + observe
- Refer to thoracic surgeons - chest drain/thoracotomy
Location:
- Needle aspiration = 2nd ICS, MCL
- Chest drain = triangle of safety (axilla, pectoralis major, latissimus dorsi, 5th ICS) - 4th/5th ICS, MAL
Surgery:
- Open thoracotomy (or video-assisted thoracoscopic surgery = VATS)
- Follow-up surgery –> pleurodesis (mechanical abrasion/chemical irritation)
Lung cancer - epi? presentation? types? Ix? Mx?
Epi: Second most common cancer in UK
Presentation: chronic cough, haemoptysis, FLAWS
- Monophonic wheeze, pleural effusion signs (dull on percussion, reduced BS), cachexia, SVCO (face swelling & engorged veins in venal-caval distribution), hypertrophic pulmonary osteoarthropathy (HPOA)
- RFs: smoking, asbestos exposure, FHx
Types:
- Non-small cell lung cancer (MOST)
- Adenocarcinoma (MOST COMMON LC)
- Non-smoking women (40% cases)
- Squamous cell carcinoma (SCC)
- Affects large airways of lungs (central)
- Classically assoc w/ paraneoplastic hypercalcaemia, as tumour may release PTHrP
- 2nd most common in non-smokers
- Most common cause of Pancoast tumour
- Keratinization (keratin pearls)
- Large cell carcinomas (Dx of exclusion)
- Alveolar cell carcinoma = ++sputum
- Bronchial adenoma = mostly carcinoid
- Carcinoid syndrome - flushing, diarrhoea, episodes of dyspnoea
- Urinary 5-Hydroxyindoleacetic Acid (5-IAA) levels may be used to screen for carcinoid syndrome
- Adenocarcinoma (MOST COMMON LC)
- Small cell lung cancer (15%)
- Almost exclusively smokers
- Can be assoc w/ neuroendocrine syndrome (SIADH, Cushing’s)
- Early mets BUT chemo sensitive
Ix:
- Bloods - FBC, haematinics, Ca
- Imaging - CXR, CT chest (2WW referral), CT PET scan (staging, mets)
- Interventional if suspicious CXR:
- Endobronchial US-guided biopsy (EBUS) & biopsy
- Video-assisted Tracheostomy & Biopsy (VATS - BIOPSY) of accessible nodes
Mx:
- Conservative: lung cancer MDT
- Smoking cessation
- Psych support (McMillan Nurses, specialist lung cancer nurse involvement)
- Palliative care (if terminal, Sx control & planning)
- Medical:
- Systemic chemo - esp. for small cell lung cancer (chemosensitive)
- Adjuvant/radical radiotherapy
- Surgical - if NSCLC
- VATS-lobectomy
- Open lobectomy/Pneumonectomy
4Ps of respiratory conservative Mx?
Persuade to stop smoking
Pul rehab
Prick them - influenza + pneumococcal vaccine
Psych issues
Fine vs coarse creps?
Vesicular vs bronchial breathing?
FINE (inspiratory) – pulmonary oedema (HF), interstitial lung disease (pul fibrosis)
- Best heard at base of lungs
COARSE (insp & exp) – bronchiectasis, COPD (chronic bronchitis), pneumonia
- No specific area of lungs louder
Vesicular - inspiratory > expiratory
Bronchial - inspiratory = expiratory
IHD - RFs? Types? Definition? Dx? Mx? Complications?
RFs: HTN, DM, Smoking, FHx IHD, Hypercholesterolaemia
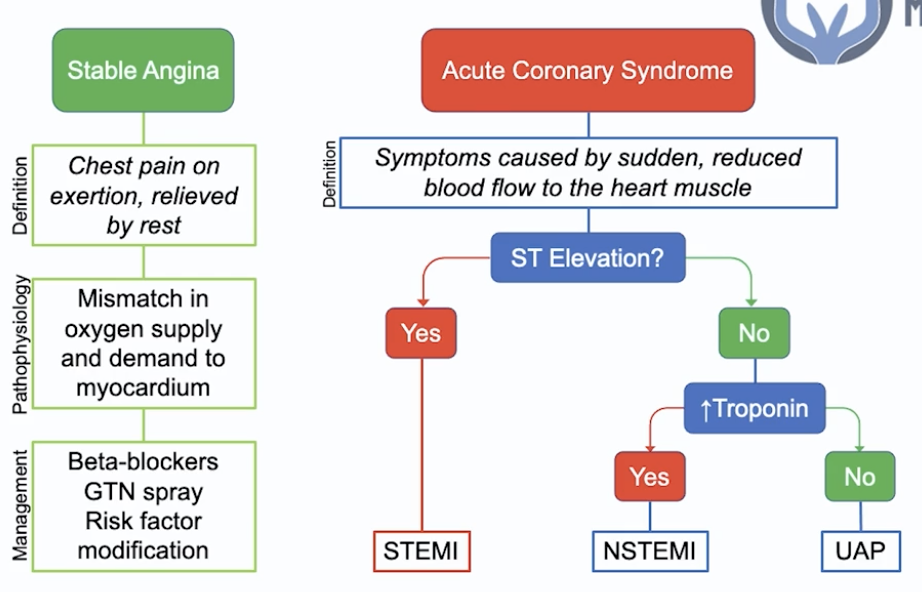
Stable angina - chest pain on exertion relieved by rest
- Path - mismatch in O2 supply and demand to the myocardium
- Ix: CT-angiogram
- Mx:
- B-blockers - reduces HR req for activity –> reduced likelihood of mismatch in O2 supply & demand
- GTN spray - reduce myocardial preload + reduces strain
- RF modification –> reduced risk of progression
Acute coronary syndrome - Sx caused by sudden reduced BF to the myocardium
- Dx:
- ST-elevation = STEMI
- Troponin raised = NSTEMI (+ dynamic T-wave inversion, ST depression)
- Unstable angina pectoris (pain at rest) = ischemia NOT infarct
- Generic ACS Mx - MONA BASH
- ALL immediate:
- 5-10mg Morphine IV + Nitrates (GTN spray)
- Dual antiplatelet therapy (DAPT) - 300mg Aspirin STAT + 300mg Clopidogrel STAT (or 180mg PO Ticagrelor)
- ALL long-term:
- Continue DAPT
- 1 year: 75mg OD Aspirin + 75mg OD Clopidogrel (or 90mg BD Ticagrelor)
- >1yr - 75mg OD Aspirin
- B-blocker (1.25-10mg Bisoprolol OD)
- ACEi (1.25-10mg Ramipril OD)
- Statin (80mg Atorvastatin OD)
- Continue DAPT
- ALL immediate:
- STEMI Mx: establish coronary reperfusion ASAP
- Sx <12hrs: PCI BUT if no PCI within 2hrs Dx –> thrombolysis (e.g. tPA - tissue plasminogen activator)
- Sx >12hrs: invasive coronary angiography ± PCI if needed
- PCI:
- If having PCI give Prasugrel (instead of Clopi/Ticagrelor)
- PCI accessed via radial (or femoral) artery, guidewire passed via X-ray guidance into the affected coronary artery AND IV unfractionated heparin during the procedure –> stent inserted impregnated with an anti-proliferative agent (e.g. Tacrolimus - to prevent adverse tissue reaction) –> takes longer for endothelialization of stent so DAPT needed for 1yr
- If PCI with stents inserted –> DAPT 12 months
- NSTEMI Mx:
- 2.5mg SC Fondaparinux (direct factor 10a inhibitor)
- Risk stratify - GRACE criteria (& others)
- High risk = invasive coronary angiography (within 48-72hrs)
Complications: FAP (failure, arrhythmias, pericarditis)
- Heart failure, arrhythmias (incl. VF)
- Pericarditis
- Early - positional chest pain day after MI –> give NSAIDs
- Late - Dressler’s syndrome - immune response @6wks (fever, pleuritic chest pain, pericarditis/pericardial effusion)
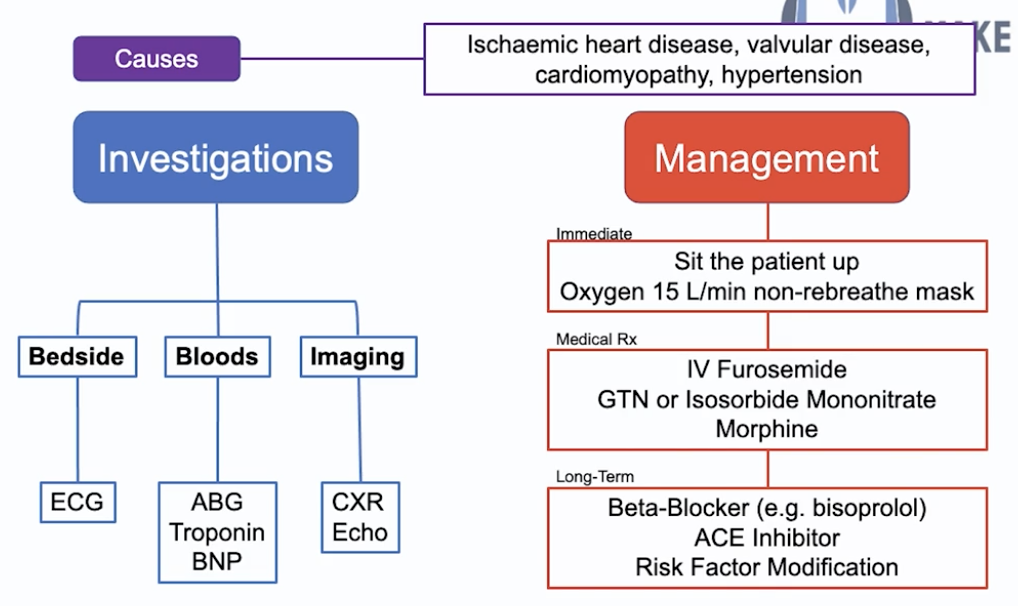
Heart failure def? Causes? Pathophysiology? Categories & Causes? Classification? Ix? Mx?
Def: pumping of blood by heart insufficient to meet the demands of the body
Causes:
- RVF:
- Acute: MI, inf endocarditis, PE
- Chr: Cor pulmonale, LVF
- LVF:
- Acute: MI, inf endocarditis
- Chronic: ischaemic/hypertensive CMO, valvular HD
Pathophysiology:
- RHF - right side of the heart pumps deoxygenated blood from the body to the lungs to be reperfused - if the RH is not pumping effectively you get the fluid collection in the peripheries = PERIPHERAL OEDEMA
- LHF - left side of the heart pumps oxygenated blood from the lungs to the body - if the LH is not pumping effectively you pooling of blood in the lungs = PULMONARY OEDEMA
- Reduced CO –> shock, tachycardia, AKI
- CO = SV*HR
- Ejection fraction = SV/End-diastolic Volume
Categories:
- HF w/ preserved ejection fraction (left ventricular >50%) = inadequate filling of ventricles during diastole (from ventricular stiffness)
- Causes of ventricular stiffness:
- Volume overload (valve regurg)
- Pressure overload (HTN)
- Decreased distensibility (constrictive pericarditis)
- Causes of ventricular stiffness:
- HF w/ reduced ejection fraction (left ventricular <40%) = inadequate emptying of ventricles during systoles (from outflow obstruction/impaired contractility)
- Causes of outflow obstruction/impaired contractility:
- MI, Cardiomyopathy, Arrythmia
- Causes of outflow obstruction/impaired contractility:
NYHA classification:
- 1 - no limitation on activity
- 2 - comfortable at rest but dyspnoea on ordinary activity
- 3 - marked limitation on ordinary activity
- 4 - dyspnoea at rest
Ix:
- Bedside: ECG - detects if anything precipitating HF (arrhythmia/ischaemic event)
- Bloods: ABG (if resp compromise from pul oedema), troponin (ACS), BNP (HF screening)
- Imaging: CXR (visualise pul oedema, cardiomegaly), ECHO (valvular abn/regional wall mov abn)
Mx: MON BA (out of MONA BASH)
- Immediate:
- Sit the patient up (reduce venous return to heart –> less strain)
- O2 15L/min NRM
- Medical:
- IV furosemide (loop diuretic) - remove excess fluid + venous dilation (reduce preload)
- Nitrates (GTN/Isosobide Mononitrate) AND Morphine - reduce preload on the heart
- Long-term:
- Reduced ejection fraction - prognostic benefit:
- B-blocker (bisoprolol) - reduce strain on heart, do not give acutely if severe HF as will kill them
- ACEi - reduce strain on heart
- After the above if LVEF <35% & Sx –> mineralocorticoid antagonist e.g. spironolactone
- 3rd line - by specialist: Sacubitril/Valsartan (entresto), Ivabradine & CRT
- SGLT2 inhibitors (dapagliflozin)
- RF modification - poor glycaemic control/high cholesterol
- Sx (diuretics)
- Reduced ejection fraction - prognostic benefit:
Complications:
- Reduced CO (SV*HR) –> shock, tachycardia, AKI
- Congestion –> pulmonary oedema + peripheral oedema
SVT - Def? Types? Presentation - case example? Mx?
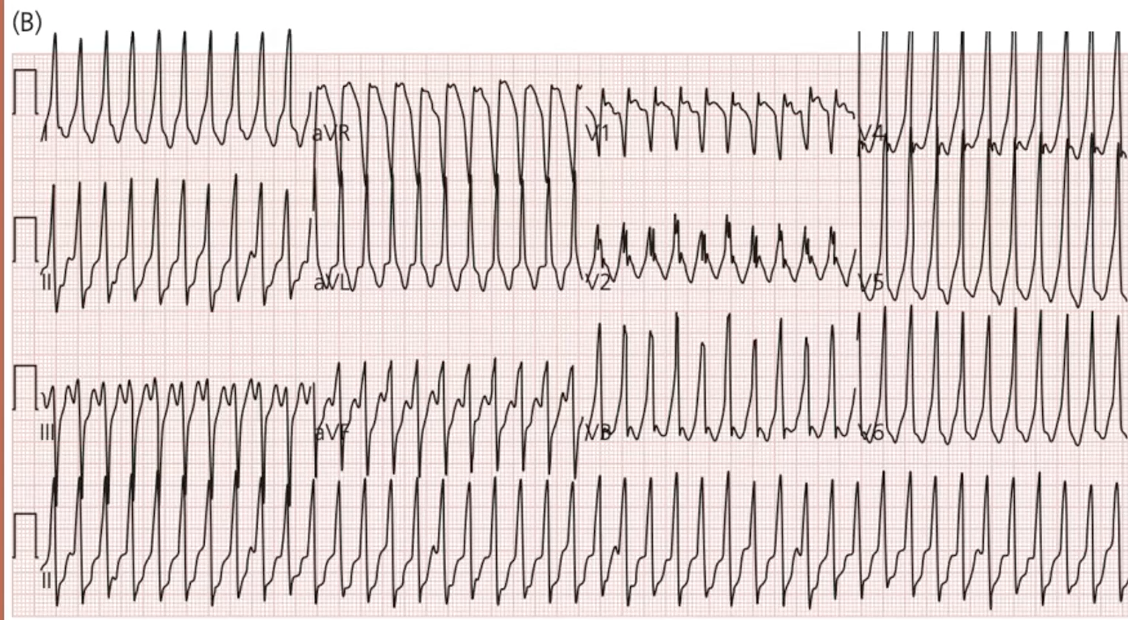
Def: regular narrow-complex tachycardia with no p-waves + supraventricular origin
Junctional types:
- AVNRT - local re-entry circuit within AV node
- AVRT - re-entry circuit between atria and ventricles –> after SVT termination = delta wave = WPW syndrome:
- Assoc w/ HOCM
- Avoid digoxin, verapamil, amiodarone (reduce conduction down SAN –> worsen retrograde conduction –> risk of VT)
- Can use B-blocker/flecainide instead
Case example: 23yrs, 1-hr palpitations + SoB, 2 similar episodes prev following alcohol, this time severe chest pain
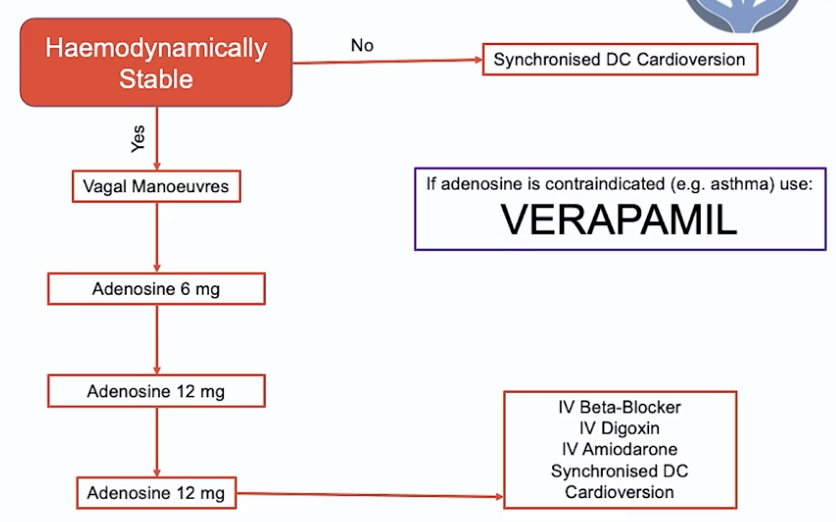
Mx:
- Unstable tachycardia (<90 BP/chest pain/acute heart failure) –> synchronised DC Cardioversion
- Vagal manoeuvres (increase parasympathetic stim via vagus nerve to slow conduction via AV node)
- Valsalva manoeuvre (blow out through nose while pinching + shut mouth) - breath through 50ml syringe
- Adenosine 6mg –> 12 mg –> 12mg
- NOTE: if adenosine CI (e.g. asthma) –> VERAPAMIL (rate-limiting CCB)
- Other:
- IV B-blocker/amiodarone/digoxin
- Synchronised DC Cardioversion
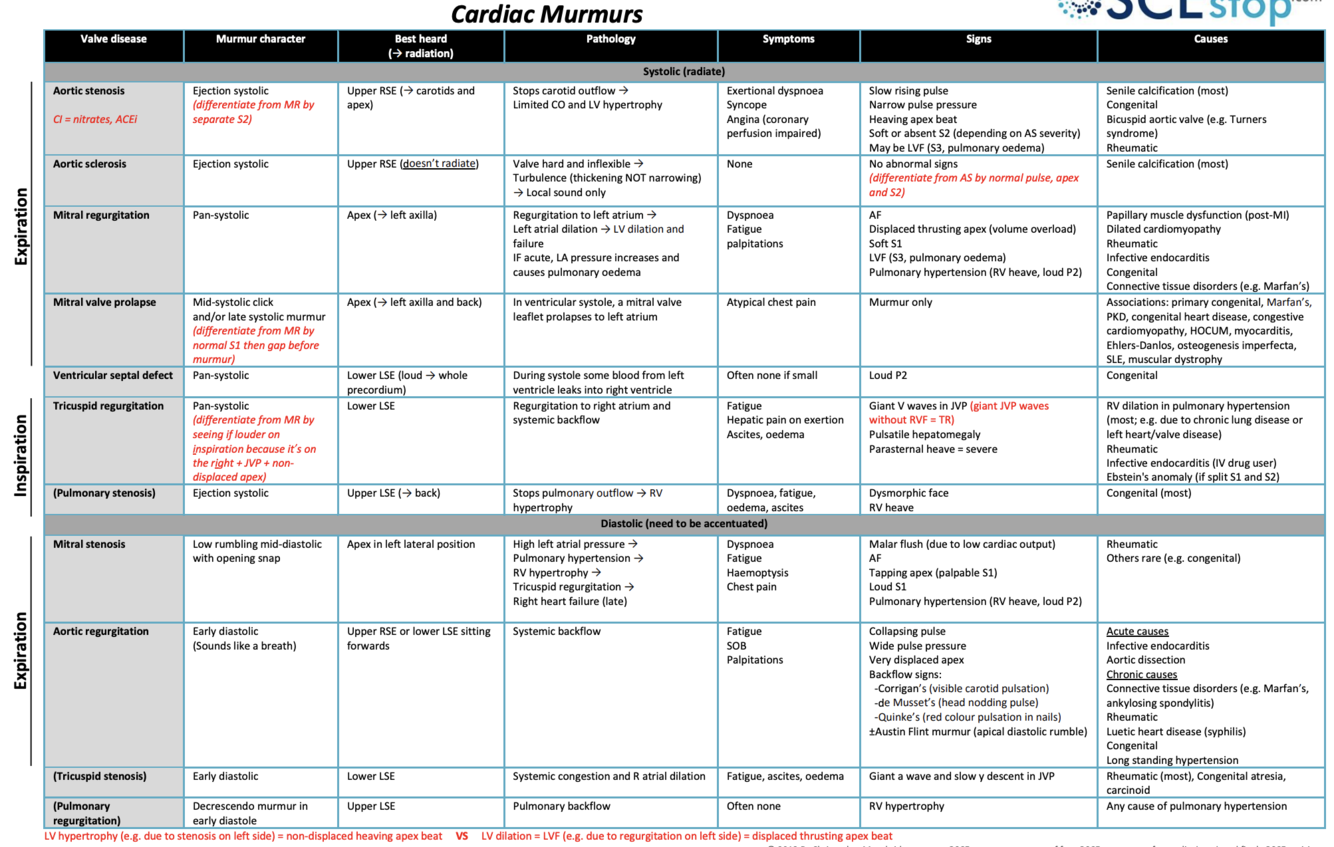
Key heart murmurs? Accentuation manoeuvres?
Causes? Left vs right heart valve abn epidemiology?
Mx? Valve types? Complications of prosthetic heart valves?
Key murmurs:
- AS = ejection systolic + radiates to carotids, slow rising pulse, narrow pulse pressure, heaving apex beat
- Sound: Wooooshhh
- Severe AS - absent/soft 2nd heart sound, reversed splitting of 2nd HS, heaving apex beat
- A longer murmur is worse (small space for blood to pass through = takes longer)
- AR = early diastolic + sitting forward (LLSE), collapsing pulse, wide pulse pressure, displaced apex
- Sound: de woooshhhh
- Severe AR –> Austin-flint murmur = ‘Rumbling mid-diastolic murmur’
- Best heard at apex, caused by blood flowing back through aortic valve and over mitral valve
- Shorter murmur is worse (quicker to flow back through large hole)
- MR = pan-_systolic_ + radiates to left axilla, AF, displaced thrusting apex, LVF/pul HTN
- Sound: Woooooshhh (holosystolic)
- MS = mid-diastolic + LLP, malar flush, AF, loud/palpable S1 “tapping” apex, pul HTN (loud P2 - pul thrill)
- Sound: Wooosh de (loud S1) de (early diastolic snap)
- NOTE: same pattern for pulmonary & tricuspid (pul stenosis & tricuspid regurgitation = systolic)
- TR - pulsatile liver
- PS - radiates to back, assoc w/ Noonan’s (AD, webbed neck, wide-spaced eyes etc.)
Accentuation manoeuvres:
- R-sided murmurs (tricuspid + pulmonary) –> louder on INspiration = blood goes IN to right-side of heart
- L-sided murmurs (aortic + mitral) –> louder on EXpiration = blood EXits left-side of heart
- AS radiates to the carotids + louder on leaning forward + listen on right sternal edge
- MS louder on turning to the left, MR radiates to axilla
Causes:
- AS (stenosis/sclerosis):
- Older - senile calcification
- Younger - bicuspid valve
- AR:
- Acute (aortic root dilation, infective endocarditis)
- Chronic (CTD, RHD, bicuspid aortic valve)
- MR:
- Acute: - IHD (papillary-muscle dysfunction post-MI), infective endocarditis, RHD
- Chronic - myxomatous degeneration (can be assoc with Marfan’s/Ehlers-Danlos)
- MS: rheumatic heart disease (RHD)
Left vs Right valve abn:
- Left = more common as higher pressure system, more likely in damaged valves, commonly Strep Viridans
- Right = more common in IV drug users –> tricuspid valve is first valve reached, commonly S. aureus
Ix:
- ECHO (Dx & severity) - Transthoracic incl doppler (regurg jet) ± TOE
- If the above is inconclusive:
- 2nd - Cardiac MRI - analysis of cardiac function
- 3rd - Cardiac catheterization (invasive) - pressure gradient
- If the above is inconclusive:
- ECG (LVH), CXR (pul HTN)
Management:
- AS:
- C: Asymptomatic –> monitor (6 monthly ECHO)
- S: Symptomatic –> aortic valve replacement:
- Fit (req midline sternotomy & cardiopul bypass) = Surgical aortic valve replacement (SAVR)
- Not fit = Transcatheter aortic valve implantation (TAVI)
- M:
- HF Sx (diuretics, ACEi)
- RF optimisation (statins, HTN, DM)
- AR:
- If no left ventricular dysfunction –> medical Mx
- ACEi, vasodilators e.g. nifedipine/hydralazine (if HTN)
- If left ventricular dysfunction & low surgical risk/another indication for cardiac surgery –> aortic valve surgery (replacement > repair)
- If no left ventricular dysfunction –> medical Mx
- MR - primary (valve abn/damage):
- Mitral valve surgery (repair > replacement)
- Medical - ACEi, B-blocker & diuretics
- Tx AF if present (incl. anticoagulate)
- MS:
- C: If non severe + asymptomatic –> monitor
- S: Otherwise = Balloon valvuloplasty/mitral valve replacement
- if C/Is (persistent left atrial thrombus/rigid calcified valve) –> need open surgery
- NOTE: valvuloplasty = lateral thoracotomy scar
- M: Tx AF if present (incl. anticoagulate)
Valve types:
- Tissue valve - porcine xenograft
- For older patients & females of childbearing-age - lasts 10-15yrs, less if active
- No need for Warfarin
- Mechnical valve - quiet clicking noise
- Younger people (<60yrs) - no need for repeat surgery, last 30yrs+
- Lifelong Warfarin
Complications of prosthetic heart valves: FIBAT
- Failure
- Infection
- Bleeding - MAHA
- Anaemia
- Thromboembolic phenomena
Atrial fibrillation (AF)
- Def? Causes? Ix? Mx?
Def: rapid, chaotic, and ineffective atrial electrical conduction
- ECG def: irregularly irregular narrow complex tachycardia with no p waves
Causes: idiopathic, cardio (IHD, valvular disease, cardiomyopathy), resp (PE, pneumonia), hyperthyroidism, alcohol
Ix: ECG (absence of p-waves, irregularly irreg rhythm)
Mx:
- Haemodynamically unstable (≤90 BP, chest pain, acute HF) –> DC Cardioversion
OR
- Rate control –> B-blocker (bisoprolol) OR rate-limiting CCB (verapamil - asthma)
OR
- Rhythm control - ONLY if clear reversible cause
- Sx onset <48hrs –> DC/chemical cardioversion (amiodarone/flecanide)
- NOTE: IV heparin started prior to cardioversion
- Sx onset >48hrs –> anticoagulate for 3wks –> elective cardioversion (also anticoag for 4wks after)
- Sx onset <48hrs –> DC/chemical cardioversion (amiodarone/flecanide)
AND
- Stroke risk - CHADS-Vasc Vs Orbit/HAS-BLED score –> DOAC (Apixaban)
- If metallic heart valve –> warfarin INR 3-3.5
- Otherwise DOAC
- NOTE: if incidental non-symptomatic AF - normal rate, no other RFs, CHA2DS2-VASc 0 –> anticoagulation not recommended
- CHF, HTN, Age ≥75rs (2), DM, Stroke (2), Vascular disease, Age 65-74, Sex - female
- Score 1 - consider; ≥2 - DOAC/Warfarin needed
- Lifetime risk = annual risk x estimated years of life left (up to 80 yrs e.g. if 60 then x annual risk by 20)
Infective endocarditis - RFs? Ix? Dx criteria? Mx?
Acute vs subacute bacterial endocarditis - what hearts affected? who are commonly affected? What bacteria most likely?
Def: infection of heart valves (typically mitral/aortic or tricuspid in IVDU)
RFs: bacteraemia (long-term lines, IVDU, dental work), abn valves (prosthetic, RHD), prev endocarditis, VSD, piercings
Presentation: low-grade fevers, night sweats
- Exam:
- Splenomegaly
- Splinter haemorrhages, osler’s nodes, Janeway lesions, petechiae, Roth spots (eyes)
- Chronic = clubbing (rare, mostly acute now)
Ix:
- Urine dip - haematuria
- Serial BCs (x3 but start empirical abx), ESR
- Transoesophageal Echo (TOE - vegetations)
Dx: DUKE’S CRITERIA (2 major OR 1 major + 3 minor OR 5 minor):
- Major: +ve BC (typical organism), new regurg murmur/veg on echo
- Minor: RF, fever (>38), embolic (vascular) phenomena, immune phenomena, +ve BC (another organism)
- Mx: IV abx for 6wks – fluclox/vanc/gent
Acute in structurally normal heart – In IV drug user the first valve met is tricuspid valve, commonly S. aureus (also most common cause in prosthetic valve endocarditis)
Subacute in structurally abn heart – mitral & aortic valves more commonly affected as high pressure system, more likely damaged valves, commonly Strep Viridans (overall most common cause of endocarditis)
3rd & 4th heart sounds - sounds & cause?
3rd = rapid ventricular filling = volume overload e.g. HF (reduced EF/systolic)
- KEN…TU.CKY (deee. de.de)
4th = atrial contraction against stiff ventricles = pressure overload e.g. longstanding AS & other causes of left ventricular hypertrophy (HTN heart disease, HOCM, HF with preserved EF/diastolic)
- TE.NE..SSEE (de.de.deee)
2 days of chest pain following 4 days of generalised muscle aches
- Worse on inspiration & lying flat
- Low-grade fever
- Exam: pericardial rub
Causes? Dx? Ix? Mx?
Pericarditis
Causes:
- Viral (most common)
- MI (can be Dressler’s syndrome)
- TB (constrictive)
- Uraemia (CKD where urea high –> pericarditis) = indication for haemodialysis (HUMP)
- Hydralazine (AI pericarditis)
- NOTE: also causes drug-induced lupus
- SLE, RF, radiation
Presentation:
- Pleuritic chest pain, worse lying flat
- Exam: pericardial rub - “creaking/scratching”
- Tip - put on all-fours, put stethoscope on sternal edge, hold inspiration
Ix:
- ECG: ST elevation widespread
- Only slightly raised/normal troponin
Mx: colchicine (3 months) + NSAIDs (ibuprofen, max 2wks)
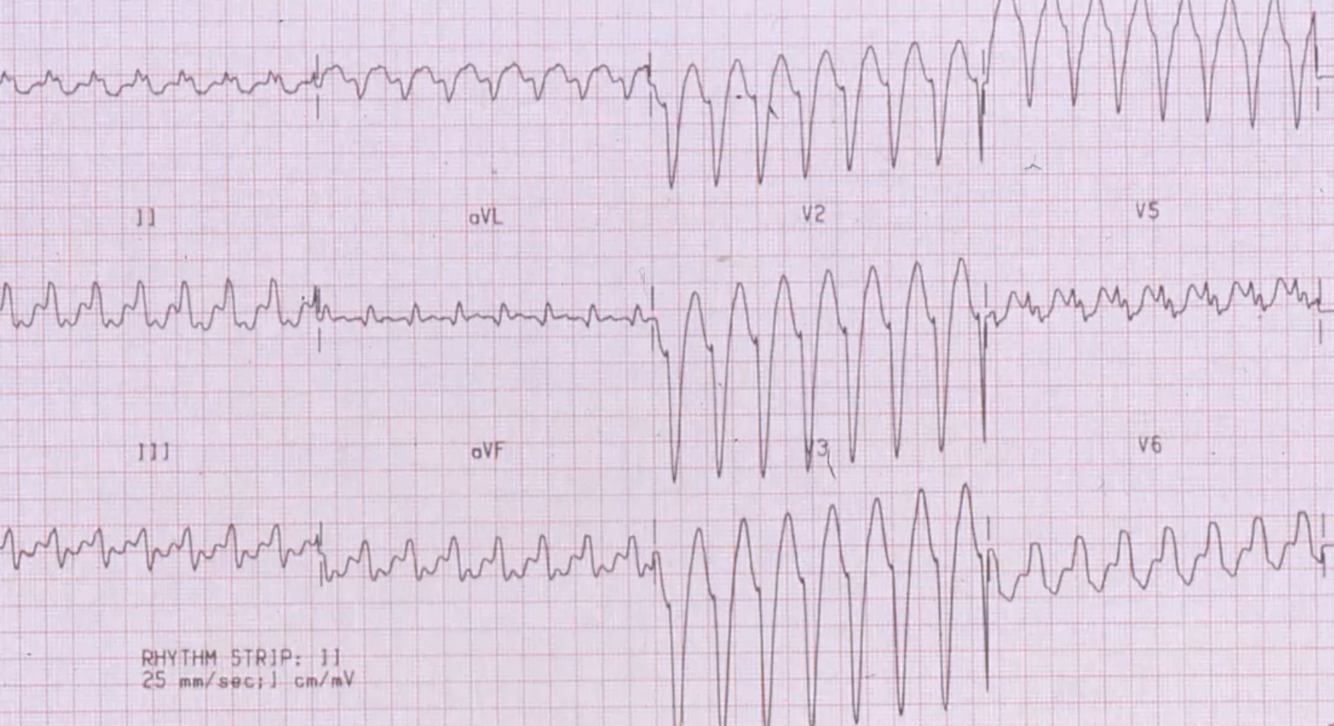
Ventricular tachycardia - Dx? Presentation? Ix - appearance on ECG? Mx?
VT or SVT w/ aberrancy
- SVT >200bpm, also often irregular
- VT more likely if LAD
- Acutely treat any broad complex tachy as VT until proven otherwise
Presentation: palpitations, light-headed, chest pain, syncope, seizure
- Tachycardia, LVF
- ACS most common cause
- NEVER IGNORE palpitations & light-headedness
Ix: ECG - regular broad complex tachycardia
- U&E (Mg, Ca, K), TFTs, Troponins
Mx:
- Unstable tachycardia (BP <90, chest pain, acute cardiac failure) = DC cardioversion
- Stable:
- IV amiodarone, b-blocker –> prepare for DC cardioversion
Bradycardia arrhythmia with a palpable pulse (peri-arrest) - Mx?
Innitial: A-E
- If unstable - 500mcg IV atropine (/5mins up to 3mg)
- Also considered unstable if:
- Recent asystole >3s/Mobitz T2 AV block/3rd degree heart block
- Caution in acute MI, C/I if heart transplant
- Also considered unstable if:
- If persistent –> transcutaneous pacing + analgesia/sedation (very painful)
- If can’t be achieved properly –> IV isoprenaline/adrenaline (specialist help)
- Arrange transvenous pacing (temporary if recent asystole >3s/Mobitz T2 AV block/3rd degree heart block)
Heart block causes? types? Ix? Mx? Complications?
Causes:
- MI/IHD (MOST COMMON)
- Inf (RHD, IE)
- Drugs (digoxin)
- Metabolic (hyperkalaemia)
- Infiltration of conducting system (e.g. sarcoidosis)
- Degeneration of conducting system
Types:
- First Degree AV block - fixed prolonged PR interval (> 0.2 s) - ASYMPTOMATIC
- Second degree AV block:
- Mobitz TI (Wenckebach) - progressively prolonged PR interval –> P-wave NOT followed by a QRS complex = ‘going, going, gone’
- Normally asymptomatic
- Mobitz Type II - intermittently P wave NOT followed by a QRS
- May be regular pattern of P waves not followed by QRS (e.g. 2:1 or 3:1)
- Can cause:
- Stokes-Adams Attacks (syncope caused by ventricular asystole)
- Dizziness, palps, chest pain, HF
- Mobitz TI (Wenckebach) - progressively prolonged PR interval –> P-wave NOT followed by a QRS complex = ‘going, going, gone’
- Complete AV heart block - no relationship between P waves and QRS complexes
- Presentation as in Mobitz T2
Ix: ECG
- Bloods: TFTs, Digoxin, cardiac enzymes (troponin, CK, BNP)
- CXR (cardiac enlargement, pulmonary oedema)
- Echo (wall motion abn, aortic valve disease, vegitations)
Mx:
- Acute block - if clinical deterioration:
- IV atropine
- Consider temporary transcutaneous pacing
- Chronic block:
- 1st degree monitored
- Permanent pacemaker in:
- Symptomatic Mobitz T1
- Advanced Mobitz T2
- Complete heart block
Complications: asystole, cardiac arrest, HF, surgical complications of pacemaker insertion
Types of pacemaker? When to use each type? Complications?
Types:
- Implantable Cardioverter Defibrillator (ICD, has a thicker end)
- Single-chamber pacemaker (right ventricle)
- Used in permanent AF (no organised atrial contraction so atrial lead not required to sense contraction)
- Rarely can have atrial lead only - if SA disease in young with good AV conduction
- Dual-chamber pacemaker (right atrium & ventricle)
- Can have ICD dual-chamber pacemaker
- Used in paroxysmal AF/all other scenarios (there is sometimes organised atrial contraction - this is sensed by the atrial lead)
- Cardiac Resynchronisation Therapy/Biventricular pacemaker (right ventricle, left ventricle ± right atrial lead)
- Can have ICD biventricular pacemaker
When to use each type:
- Atrial lead only → Sino-atrial disease in young people with good AV node conduction
- RV lead only → Pacing whilst in permanent atrial fibrillation
- Dual-lead → All other scenarios (paroxysmal AF, bradycardia)
- CRT → LV dysfunction + broad QRS –> end-stage HF
- Indications for ICD:
- Primary prevention = @risk of serious ventricular arrhythmia
- Familial cardiac conditions (hypertrophic cardiomyopathy, long QT)
- Previous surgical repair of congenital HD
- Previous MI + LVEF <35% + HF Sx
- Secondary prevention = had previous serious ventricular arrhythmia wo/ treatable cause
- Cardiac arrest from VT/VT
- Spontaneous sustained VT AND:
- Syncope/haemodynamic compromise OR
- LVEF <35% + sign HF Sx (NYHA 3+)
- NOTE: VT/VF from STEMI has treatable cause (open occluded vessel)
- Primary prevention = @risk of serious ventricular arrhythmia
Complications:
- Surgical complications - infection, bleeding, damage to underlying structures
- Displacement (of lead)
- Pacemaker syndrome (if ventricular lead with no atrial) –> AV node conducts in retrograde direction = mitral/tricuspid regurge + HF Sx
How do you know this is the JVP and not the carotid pulse?
- Not palpable
- Double pulsation
- Obliterated when pressure applied at base of neck
- Rises with hepatojugular reflux
- Height changes with respiration















































-
Respiratory_Medicine26
-
Cardiology_Medicine24
-
Gastroenterology_Medicine & Surgery42
-
Neurology_Medicine & Surgery41
-
Endocrinology_Medicine17
-
Musculoskeletal_Medicine30
-
Renal_Medicine & Surgery12
-
Dermatology_Medicine7
-
Haematology_Medicine13
-
Emergency Medicine23
-
Instruments69
-
Vascular, Breast & Thyroid Surgery18
-
PACES Exams19
-
PACES ALL212
-
PACES ALL concise111
