A patient presents with hematuria and oliguria. Kidney biopsy with silver stain is shown below.
- What is the diagnosis?
- The abnormal deposition is made up of what?
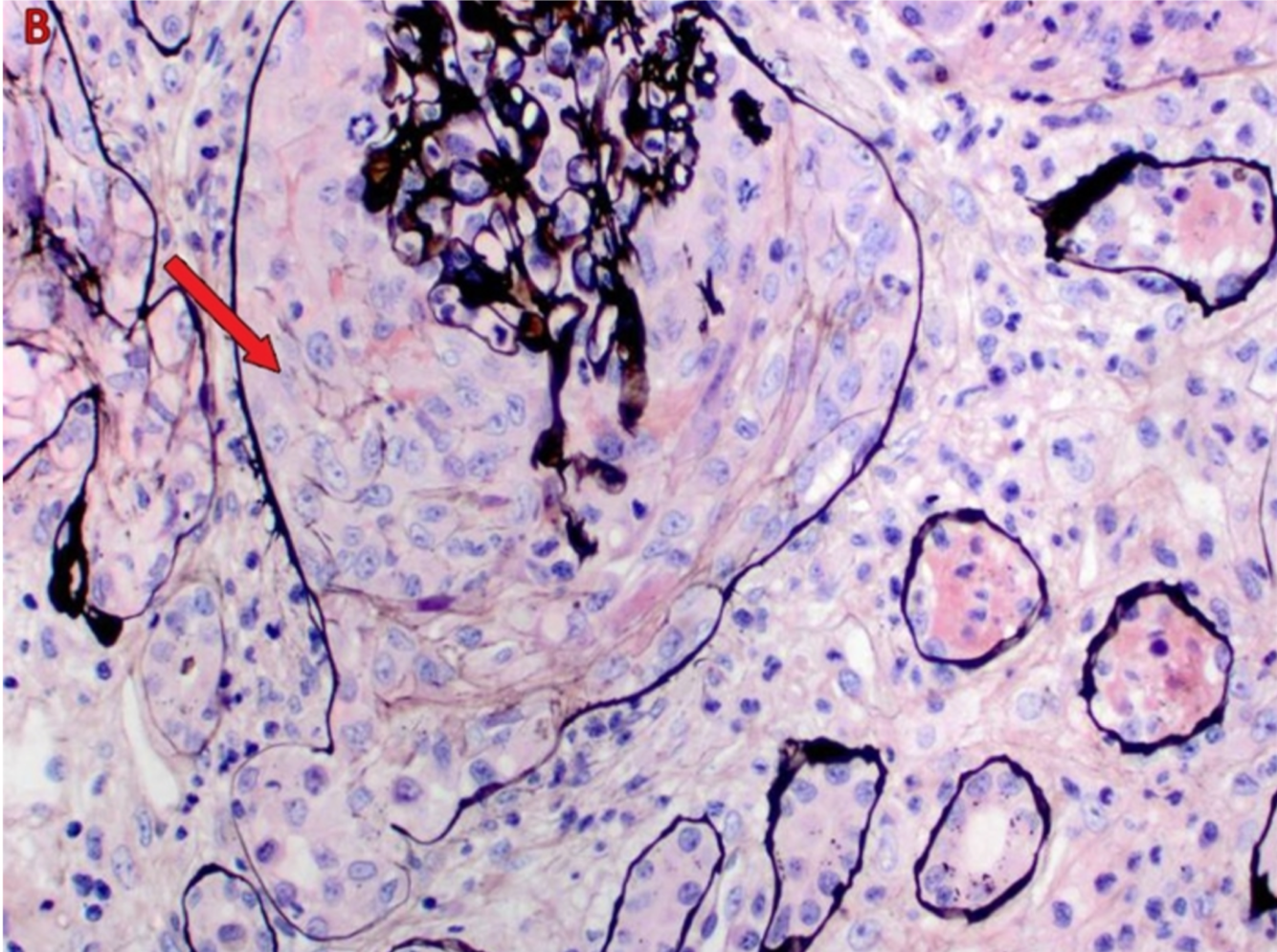
- Rapidly Progressive Glomerulonephritis
(crescents in bowman space)
- Crescents are filled will fibrin and macrophages
A biopsy of a cancerous lung lesion is shown below.
Where did this cancer originate from and why?
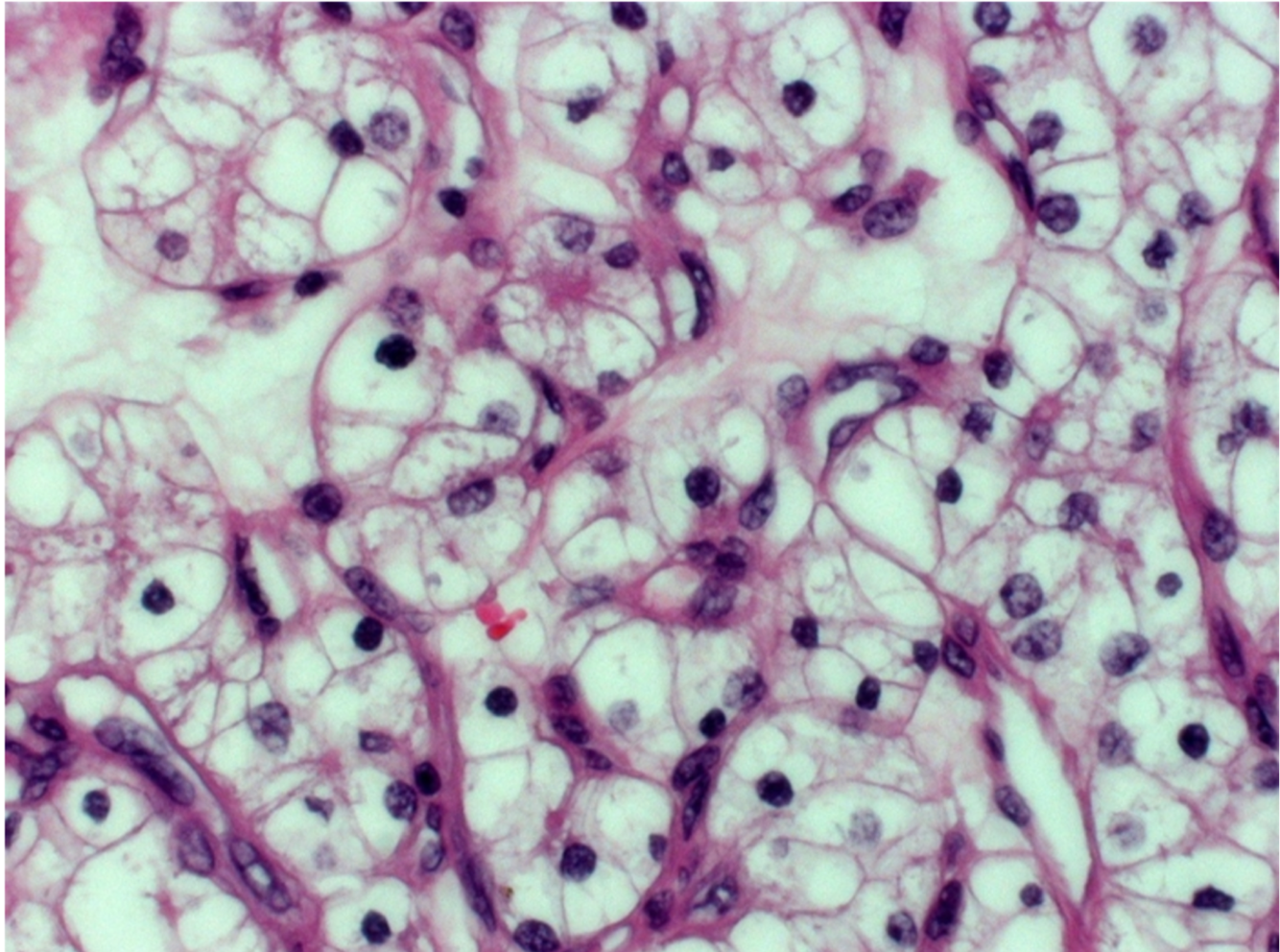
The Kidneys (renal cell carcinoma)
Due to the empty/clear cytoplams
(clear cell renal carcinoma - most common type)
How and does Benign Prostatic Hyperplasia affect the ability to urinate? Why? Major complication?
It increases resistance to urine flow due to compressing the urethra (increasing the hydroostatic pressure required to overcome resistance to flow)
This results in incomplete emptying of the bladder.
(as bladder empties urinary pressure will soon fall below the bladders leaving a residual volume of urine)
Most common complication is UTI
In poststreptococcal glomerulonephritis (PSGN) what is the most important poor prognostic factor?
Increased Age
In a patient recovering from acute tubular necrosis, what is the major complication and why?
Major complication: Electrolyte Imbalances + Oliguria
(hypokalemia, hypocalcemia, hypophosphatemia)
This occurs due to GFR improving before tubular cell recovery
(tubular cells are stable cells and take some time to reenter cell cycle)
How would the following be altered in a hypovolemic patient in comparison to a regular person:
- RPF (renal plasma flow)
- GFR (glomerular filtration rate)
- FF (Filtration Fraction)
1. RPF is decreased
(RPF = amount of blood going to kidneys)
2. GFR is decreased
(GFR = amount of filtered blood in kidneys)
3. FF is increased
(FF = GFR/RPF)
(FF is increased during hypovlemia to try to maintain GFR)
Which toxic agents can result in Acute Tubular Necrosis?
- Aminoglycosides (ex: gentamycin)
- Heavy metals (ex: lead)
- myoglobinuria (ex: from crush injury to muscle)
- ethylene glycol/antifreeze
- radiocontrast dye
- urate (used for chemotherapy, prevented by also giving allopurinol)
How can Heart Failure affect the renal system?
Cardiorenal Syndrome
- HF results in decreased renal perfusion
- Activation of RAAS + ADH release + sympathetic stimulation
- Na and H2O reabsorption and systemic vasoconstriction
- Exacerbation of HF and further renal hypoperfusion
How would hypovolemia affect the following:
- Vasopressin
- Norepinephrine
- Angiotensin II
- Endothelin 1
All will be increased
In minimal change disease, what are the effects of albumin loss on:
- Plasma Oncotic Pressure
- Lipoprotein production
- decreased plasma oncotic pressure
- increased lipoprotein production –> hyperlipedemia
(stimulated by decreased oncotic pressure)
In acute tubular necrosis, which structures are most susceptible to ischemic damage?
- medulla
- proximal tubule
- thick ascending limb
How would uterolithiasis (stone in ureter) present?
- hydronephrosis (swelling of kidney due to build up urine)
- Hematuria (RBCs with no RBC casts)
- Stone crystals
How/why does Osteodystrophy occur with chronic renal disease/failure?
- Impaired renal fcn –> hyperphosphatemia + hypocalcemia
2. Increased PTH (secondary hyperparathyroidism)
3. Increased osteoclast function
4. Osteodystrophy
What is the earliest sign of diabetic nephropathy?
Albuminuria
What are 2 general things that can decrease renal stone formation?
- Increased fluid intake
- increased urinary citrate
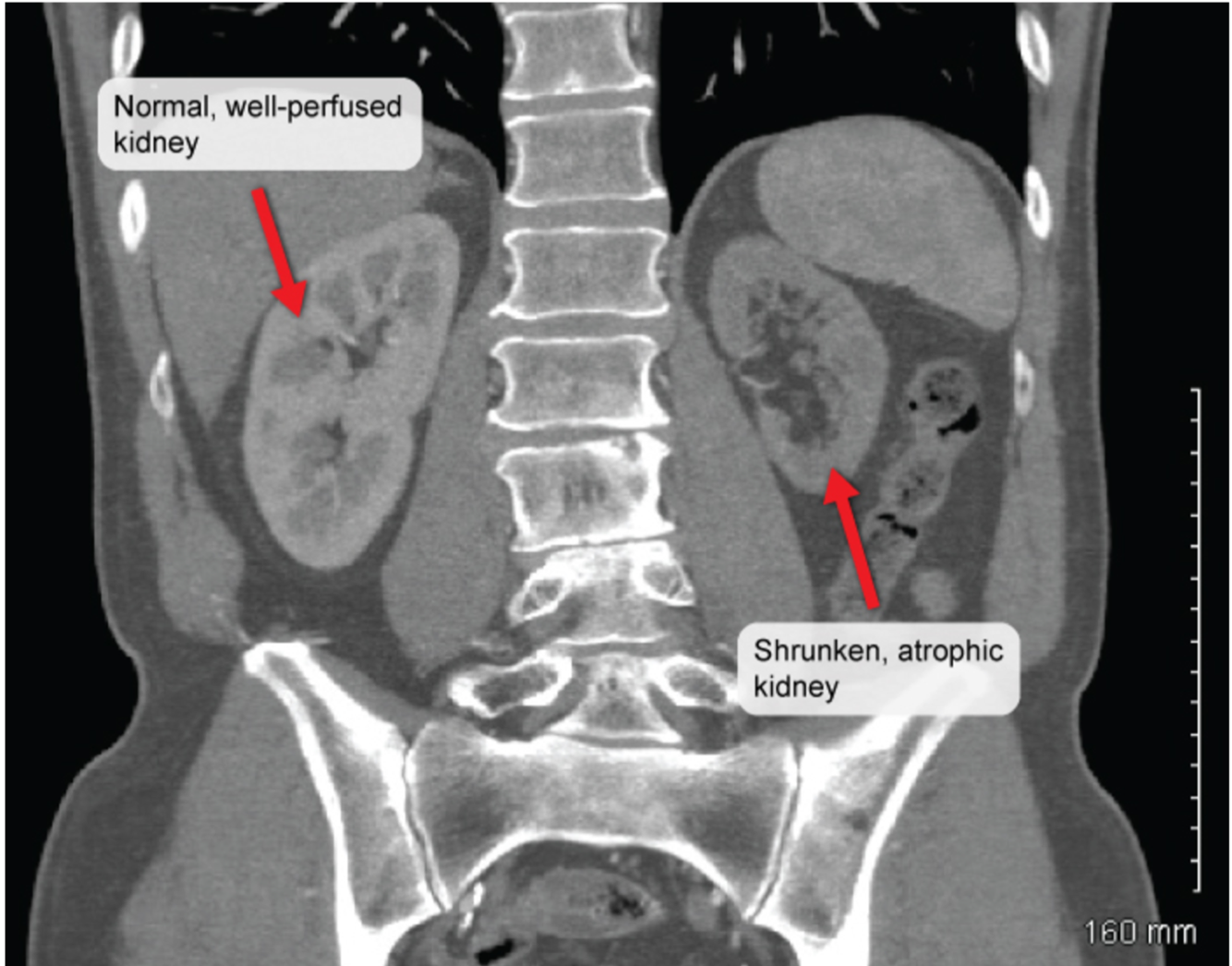
A 65 yo patient comes in complaining of abdominal pain after eating who has a BP of 175/110.
CT scan of the abdomen reveals the following:
What condition is this patient most likely suffering from?

Renal artery stenosis
- marked unilateral kidney atrophy
- commonly occurs in elderly with other atherosclerotic diseases (in this case: mesenteric ischemia)
How can chronic kidney disease cause spasms?
- impaired kidney function results in hyperphosphatemia
2. Phosphate binds calcium
3. hypocalcemia
4. spasms
IgA Vasculitis / Henoch-Schonlein Purpura
- What is it?
- Who comonly gets it?
- How does it present?
- Small vessel vasculitis due to IgA immune complex deposition
- Most commonly occurs in children
3.
- palpable purpura on buttocks
- GI pain + bleeding
- joint pain
- Hematuria
Interstial Nephritis
- What is it?
- What can cause it?
- How does it present?
- What can it progess to?
- Drug-induced hypersensitivity that results in acute renal failure (intrarenal azotemia)
- P’s
Diuretics (Pee), NSAIDs (Pain-free), Penicillins, PPIs, RifamPin
- Oliguria, fever, rash (eosinophils may be present in urine)
- Renal Papillary necrosis
Renal Papillary Necrosis
- How does it present?
- What causes it?
- Flank pain and Hematuria
- “SAAD”
Sickle cell disease/trait
Acute Pyelonephritis (kidney infection)
Analgesic/NSAID abuse
Diabetes
How can BPH damage the kidney structure?
- BPH blocks prostatic urethra
- Hydronephrosis occurs
- Build-up of urine causes parenchymal pressure atrophy of kidney
IgA Nephropathy (Berger’s Disease)
- Clinical presentation?
- Microscopic Presentation?
- hematuria that occurs following a mucosal infection
2. IgA deposition in mesangium of glomeruli
Hemolytic Uremic Syndrome
- What is the classical ‘triad’ presentation?
- What causes the kidney effects?
1. Triad of:
- Thrombocytopenia
- Microangiopathic Hemolytic Anemia
- Acute Kidney Injury
2. Acute kidney injury occurs due to microthrombi in small blood vessels
How would the following values in a patient with long-standing Polycysitic Kidney Disease compare to a healthy individual:
- Phosphate
- PTH
- Calcitriol
Chronic Kidney Disease (in this case PKD) results in:
- Phosphate is increased (causes hypocalcemia)
- PTH is increased (to try and increase Ca levels
- Calcitriol is decreased
(even though it functions to increase Ca, it is inhibited by phosphate)











