Phillips - Pregnancy Flashcards
(144 cards)
What things need to happen to make L and D successful?
- Review records for medical problems, risk factors: ex, GBS+ patient will get penicillin during labor
- Routine labs: CBC, type/screen for blood products
- IVF: D5LR for fluid replacement
- Anesthesia consult for epidural: discuss this prior to delivery (bedridden following administration)
1. NO total pain relief, so pts should be ready for some degree of pain and discomfort - Pitocin (dilute solution) almost routine: promotes normal contraction pattern (pts may abstain)
- NPO in labor process, but frowned upon in some more “natural” settings: DEC risks w/ anesthesia
- Comfort, and questions answered
What kind of monitoring is done during a typical L and D?
-
Fetal monitoring: external monitors continuously
1. Freq review of fetal heart tracing: most units have central monitoring capacity via a screen w/all laboring pts and fetal HR at that time - Periodic exams (of cervix) for progress: try to keep these at a MINIMUM because more exams lead to INC risk of infection
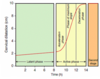
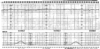
What do you see here?

- Intrapartum fetal (top) and contraction monitoring
-
FHR: baseline 132 bpm; moderate variability (normal: external monitoring)
1. Qualitative, not quantitative if external
2. Quantitative FHR on time: variability normal, even acceleration (going way above baseline) -
Contraction pattern: q3-4 minutes (normal)
1. Dark, vertical bars designate 1 minute so you can count how frequent the contractions are
2. #’s on vertical axis give you some basic info concerning contraction strength -> this can’t be measured via external monitor (body habitus), so internal monitoring via catheter in uterus can be used for better values
What is the typical recovery time for a vaginal birth?
- Recovery 24-36 hours on floor, then discharge
- Depends on pt energy level, and what kind of help she has at home
What is the estimated blood loss in vaginal birth?
- 500cc
- Very normal, considering that pt goes into labor process with 40-50% excess cardiac volume
What is an episiotomy? Is it routine in vaginal birth?
- Episiotomy: incision in vagina to allow room for baby to come out
- NOT routine, although it was in the past
What happens to the baby post-L and D?
- Baby in room with mom!
- Mom should be responsible for caring for baby from delivery on (with exception of small amount of time in nursery for routine blood work, etc.)
- Breastfeeding IMPORTANT
What are the indications for Cesarean birth (10)?
- Malpresentation of the fetus (breech): anything other than the head
- Failure to dilate/descend: understand labor curve, and have same person examine pt time and again (pt can’t be in labor forever)
-
Abnormal fetal heart tones: might predispose baby to lack of oxygen and acidemia, which pose risks of cerebral palsy and brain damage
1. Monitor to prevent these, and do cesarean earlier rather than later (malpractice, yo; cerebral palsy actually more complicated) - Some birth defects: NTD babies better off with cesarean delivery; gastroschisis babies CAN be born vaginally (doesn’t matter)
- Previous C-section or scarred uterus: MOST COMMON REASON -> safe to attempt vaginal birth after 1 C-section, but risks to fetus and mother of uterine rupture (risk 1%, so women given choice)
- Triplets or higher: twins can be born vaginally or cesarean, depending on presenting fetus -> if 1st is vertex, vaginal delivery; if breech, then cesarean
- Active herpes simplex virus at due date: neonatal herpes happens as baby is passing through vagina where lesion is present, producing virus -> women given prophylactic anti-virals at 26 wks gestation, so less likely moms will have outbreak near term
- High viral load and HIV: if comes in with labor or ruptured membranes, fetus already exposed, and no advantage to cesarean birth
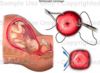
- Placenta previa: usually implants high, but if low, then covers cervical os, and C-section necessary -> high risk for bleeding, and can be emergency, requiring hysterectomy, or causing maternal death (placenta can bleed as cervix dilating)
- Patient request: remind pt there are risks assoc w/major sx, but most physicians honor this request
How common is C-section?
- Quite common:
1. <1/4th at public hospitals
2. May be up to ½ in some private hospitals - INC rate in previous decades
What do you see here? What do you want to do?
- FHR w/baseline of 170 bpm, minimal variability
-
Late deceleration: following contraction, slight downward trend of FHR, then slope upward
1. Indication that fetus might be becoming hypoxic and acidemic
2. Indication for expedited cesarean delivery to get baby out as soon as possible
How are incision/closure decided in C-section?
- Abdominal and uterine incision type depends on indication
- Type of closure and suture according to best evidence and surgeon preference
- Don’t really need to know details about these things yet
What MUST be given in the case of a C-section?
- ANTIBIOTICS REQUIRED to prevent surgical site infection
What is the estimated blood loss (EBL) in C-section? Recovery time?
- EBL: 1000cc
1. Some pts come into process with low Hct or anemic, and may need blood transfusion with this much blood loss (even though this is normal for this type of procedure) - Recovery time 24-48 hours: usually go home on post-op day 2
What are some complications associated with C-section?
- Hemorrhage
- Surgical injury to bladder/bowel: can occur
- Surgical site infection: give AB’s intra-operatively to try and prevent this
- Adhesions: prone to these, as are all pelvic surgeries
- Need for repeat CD: adhesions can present real problems in subsequent C-sections for both mom and baby (in terms of trying to get baby out)
- Try to avoid cesarean delivery if possible b/c great deal of morbidity and mortality associated
What counseling should happen post-partum (5)?
-
Lochia: vaginal bleeding/discharge persists 3-8 wks -> heavy + bloody initially, like a period; tell pt!
1. Occasionally a heavy bleed at day 7-14 pp b/c eschar (scab) at placental site sheds; warn pt this is NOT a menstrual period
2. Exercise, sex, driving, work can resume when pt is comfortable (except in extreme circumstances) - Birth control can be addressed, given in hospital
- Breastfeeding encouraged, supported in hospital and in post-partum period with lactation advisers
- Baby care: neonatology folks usually come by, and suggest 2-week return visit
- Warnings about depression: baby blues common, but depression a very serious issue -> seek attention if there are any concerns
What is post-partum depression?
- DSM-classified mental illness
- >10% of women have depression w/in first 3 mos post-partum
-
Different than ‘baby blues,’ which have to do with excitement of delivery fading, and “cheerleaders” leaving mom to fend for crying baby by herself
1. Women usually come to grips with this sort of scenario and recover just fine
What are the risk factors for post-partum depression?
- Previous episodes
- Inner city women
- Mothers of preterm babies
- Adolescent mothers
- NOTE: life stresses might make you more prone, but this illness affects people of ALL SES and ethnic gps
What kind of screening is done for PP depression?
- Routine screening on ALL moms: Edinburgh Depression Scale
- Pediatricians sometimes recognize this before OB/GYNs, who don’t see moms until about 6 wks (peds sees them at 2-4 weeks)
- Important for baby that the mom is not depressed, and care for/feeding of baby can be impacted
1. BONDING - Moms may also present to OB with specific complaints of trouble coping
What is the physiologic basis for PP depression?
- Withdrawal of hormones at delivery may be what pushes people into these depressive episodes
- People with predisposing mental illness more prone to these types of problems
What are the symptoms of PP depression?
- Crying
- Helplessness
- Exaggerated worry about baby: may stay awake to watch baby breathe
- Sleeplessness: exhaustion, crying, feeling of helplessness
- Different than baby blues, which is a realization that life is forever changed, frustrated with new duties or lack of support
What are the biggest concerns in PP depression?
- Biggest concern for baby is lack of bonding at a critical time
- Psychosis, suicide, even homicide are the biggest concersn for the mom
1. This is extreme, but it has happened
PP depression dx and treatment?
- SSRIs (Sertraline): works, safe, can be used during breastfeeding -> benefit far outweighs the risk
- Continue breast-feeding: crucial for bonding process to continue, and mom to climb out of this “helpless” state
- Frequent OB visits: seldom need psychiatric care, unless severe or has pre-existing disease, in which case they would get back with routine counselor
- Hospitalization sometimes necessary: pt will often tell you that she needs this to detach completely, recover, and come back
-
Symptoms usually remit around 8 weeks post-partum, but may continue to 3 months and beyond
1. Pt may need assistance with psychiatrist if anything out of the ordinary
Physiology of lactation during pregnancy?
- Progesterone influences growth in size of alveoli and lobes of breast tissue
- Estrogen stimulates the milk duct system to grow and differentiate
- Prolactin causes differentiation of the alveoli and ductal structures
- Human placental lactogen (HPL) produced by the placenta, and causes breast, nipple, areola to grow
What are the benefits of breast feeding for the infant?
- Passive immunity: fully functional IgA, IgG and IgM passed from mom to baby, preventing infections, and starting baby off on good foot
-
Nutrition: formula-fed have higher, faster weight gain in newborn period and INC # of fat cells (these never go away)
1. Protects against obesity - Protects against allergies/asthma
- Bonding: helps produce confident infant and child