Phys exam 2 Flashcards
(141 cards)
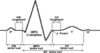
what action is responsible for the heart sounds
the valves closing makes the sound of the heart
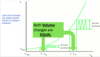
which valves are wider and why?
- AV valves
- semilunar valves
- AV valves are wider.
- semilunar valves are narrow because they need to shoot out with more pressure.
The heart does not contract simultaneously.
- What direction does it contract?
- What timing stays the same?
- it contracts from top to bottom
- then bottom to top
- Left & right stay the same, though
Define cardiac output
- what’s remains the same
- what may be different
How much does each portion get (%):
- renal
- GI
- muscles
- cerebral
- coronary + skin
- cardiac output = volume/minute
- pressure may change
- volume stays the same
- each portion
- renal, GI, muscles = 25%
- cerebral = 15%
- coronary + skin = 5%
who discovered that veins have one-way valves
william harvey
amongst the vessels (artery, arteriole, capillary, vein), which has the highest:
- velocity
- surface area
- volume
- control over BP
- velocity = aorta
- surface area = capillaries
- volume = veins
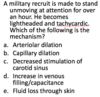
- control over BP = arterioles
Arterioles = greatest site of BP drop off
what determines the resistance of an arteriole?
- what medications constrict it?
- what medications dilate it?
smooth muscle
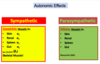
- constriction = alpha1 agonists
- dilation = beta2 agonists
- NOTE: arterioles are the only** part of the vasculature that **moves
what is the only thing that determines total peripheral resitance?
arterioles
Capillaries
- are they thin/thick
- are they fast/slow
- how many layers of endothelial cells
- are they muscular/not
Capillaries are
- thin
- slow
- 1 layer of endothelial cells
- not muscular
what function do the capillaries serve?
- what happens to lipid soluble material
- what happens to water soluble material
- capillaries are used for diffusion and picking up substances
- lipid soluble stuff goes THROUGH cells (O2, CO2)
- water soluble goes AROUND cells
what controls flow in an arteriole?
sphincters control arteriole size
- ex) pre-capillary sphincters
how many layers do arteries and veins have?
3
- endothelium
- external layer
- smooth muscle layer
what moves blood forward in veins?
name 2 differences between veins and arteries
surrounding muscles move blood forward in veins
3 differences
- they have more capacity than arteries
- they have one-way valves
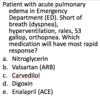
name 5 arteriole dilators (NNHPP)
name 3 arteriole constrictors (AVN)
dilating substances
- NO
- nitroglycerin
- histamine
- prostaglandins
- prostacyclins
constricting substances
- angiotensin 2
- vasopressin
- nor-epi
what’s the formula for velocity of blood flow?
Q = VA
- Q=flow
- V=velocity
- A=area (diameter)
if you take the same volume through a larger area, flow will be slower (ex: capillaries)
what happens to flow if….
- resistance goes up
- resistance goes down
- pressure at beginning goes up
what’s the major way to change flow
- high resistance = low flow
- low resistance = high flow
- high pressure = high flow
changing resistance = how to change flow
what’s Ohm’s law
Q=ΔP/R
- Q = flow
- P = pressure
- R = resistance
how does dobutamine work for patients with pulmonary embolism?
dobutamine increases pressure, therefore decreasing flow
- Q=ΔP/R
(…is this right?)
What is Poiseuille’s equation?
- what happens to resistance with
- higher viscosity
- longer tube
- narrower tube
Resistance = (Viscosity x Length) / r^4
- greater viscosity = more resistance
- longer tube = more resistance
- narrower tube = more resistancee
Using Pouisseulle’s equation for resistance, explain
- dobutamine vs. congestive failure
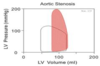
- dilating mitral stenosis
- angioplasty
- dobutamine increases pressure (force of contraction)
- this decreases TPR
- this increases the flow
- dilating mitral stenosis
- increased diameter (radius)
- -> decreased resistance
- -> increased flow
- increased diameter (radius)
- angioplasty
- use thrombolytics to increase flow
with flow, what happens if you…
- double length
- double viscosity
- double pressure
- double radius
flow when…
- double length = 1/2 flow
- double viscosity = 1/2 flow
- double pressure = 2x flow
- double radius = 16x flow
Only need 19% increase in radius to double the flow
series and parallel resistance
- what happens to total resistance with
- resistors in series
- resistors in parallel
what are all blood vessels in? (series/parallel)
- resistance in series ADDs
- resistance in parallel DIVIDEs
All blood vessels are in SERIES
- aorta to arteries to capillaries to veins
- cardiac output goes through them sequentially
- greater resistance in ONE means added resistance to the entire system
What blood vessel has the greatest variation in diameter (and thus, resistance)?
Thus, what do most BP medications target?
arterioles
- this is why most medications target arteriole diameter
- calcium blockers
- ACE inhibitors
- angiotensin receptor blockers
- beta blockers are hard to understand
- beta2 stimulation dilates
- but then why do beta blockers decrease BP?
- beta blockers decrease HR and lower renin
what will more parallel resistors do to the total resistance of a system?
more parallel resistors = lower total resistance
- adding a new ORGAN will decrease total resistance
- ex) the liver is a resistor in parallel
it’s like many toll booths
- does not mean slower flow
- does not always mean narrowing