Psychiatry - Pharmacy Flashcards
(37 cards)
Psychiatric
Pharmacy
Medication Used in Psychiatry?
- Antidepressants
- Mood stabilisers
- Antipsychotics
- Others
Psychiatric Pharmacy
Antidepressants?
- Selective serotonin reuptake inhibitors (SSRIs) – 1st choice
- Tricyclic antidepressants (TCA)
- Serotonin noradrenaline reuptake inhibitors (SNRI)
- Noradrenergic & specific serotonergic antidepressants (NaSSAs) – mirtazapine
- Noradrenaline reuptake inhibitors (NARI)
- Monoamineoxidase inhibitors (MAOI)

Psychiatric Pharmacy
Antidepressants?
Can be used for other mental health illnesses in addition to depression:
- Panic disorder
- Generalised anxiety disorder
- OCD
- PTSD
Cautious use in those with BPAD
Psychiatric Pharmacy
Anntidepressants - MOA

- Change neurotransmitters levels in the brain
- Certain neurotransmitters (i.e. serotonin and norepinephrine) can improve mood and emotion though how and why is not fully understood
- They treat the symptoms of depression, they do not necessarily address causes - usually used in combination with therapy
- ADx have to be taken for at least 3-4 weeks before they notice any improvement in their symptoms, because increasing the levels of neurotransmitters is a gradual process

Psychiatric Pharmacy
Anntidepressants - MOA
SSRIs
- Work by selectively inhibiting the reuptake of serotonin
- Most widely prescribed type of antidepressants, because they cause fewer side effects. Not addictive!
- An overdose is also less likely to be fatal
- Common side effects of SSRIs include:
- Mainly GI e.g. nausea, abdominal pain, diarrhoea (GI upset)
- Headache
- Insomnia
- Sexual dysfunction
- Anticholingeric - blurred vision, dizziness, sedation, dry mouth
- Insomnia
- Hyponatraemia in elderly
Psychiatric Pharmacy
Anntidepressants - Types of SSRIs

- Fluoxetine
- Citalopram
- Sertraline
- Paroxetine
- Escitalopram
Psychiatric Pharmacy
Antidepressants
Initiation & Discontinuation of SSRIs
- May take a few week to work (trial for at least 4-6 weeks, 6 weeks in older pts, if partial response try for another 2 weeks)
- Stop SSRIs if develop rash and must get help if agitation/suicidal feelings occur
- Patients should be reviewed 1-2 weeks after starting treatment
- After remission of symptoms, continue for at least 4-6 months (12 months in the older patient)
- Maintenance treatment may be needed in those with recurrent depression
Psychiatric Pharmacy
Antidepressants
Serotonin Syndrome

- Occurs within hours of starting SSRI or dose increase
- Restlessness
- Tremor
- Myoclonus
- Confusion
- Headache
- Rapid HR, changes in BP
- Severe cases can be life-threatening – urgent medical attention if high fever, seizures, irregular heartbeat, unconsciousness

Psychiatric Pharmacy
Antidepressants SSRIs
Discontinuation Syndrome

- Irritable/restlessness
- Nausea – “GI chills”
- Paraesthesia
- Ataxia
- Hypomania, anxiety and restlessness
- Reduce the dose gradually over about 4 weeks or so to try to avoid this. In patients who have taken the drug long-term, they may need 6 months or so to withdraw gradually

Psychiatric Pharmacy
Antidepressants
SNRIs
- Newer type of antidepressant
- Works in similar way to SSRIs but reuptake serotonin and noradrenaline
- There are currently two SNRIs prescribed in the UK:
- Venlafaxine
- Duloxetine
- Side effects, cautions and interactions are similar for both SSRIs and SNRIs
Psychiatric Pharmacy
Antidepressants
TCAs
- Older type of antidepressants
- No longer recommended as a first-line treatment
- Can be dangerous if an overdose is taken
- Cause more unpleasant side effects than SSRIs and SNRIs

Psychiatric Pharmacy
Antidepressants
MAOIs

- Older type of antidepressant with a wide range of side effects
- Only to be used if other types of antidepressants are not effective
- Need to avoid certain foods and drinks, such as red wine, older cheeses, pickled fish, which contain a protein called tyramine because consuming tyramine while taking MAOIs can cause a dangerous rise in blood pressure (cheese reaction)

Psychiatric Pharmacy
Antidepressants
Others
- Flupentixol has antidepressant properties when given by mouth in low doses. Flupentixol is also used for the treatment of psychosis
- Mirtazapine a presynaptic alpha2-adrenoreceptor antagonist, increases central noradrenergic and serotonergic neurotransmission. It has few antimuscarinic effects, but causes sedation during initial treatment
Psychiatric Pharmacy
Mood Stabilisers?

- Used to treat bipolar disorder
- They suppress swings between mania and depression
- They are also used in PD and schizoaffective disorder
- The main mood stabilisers are:
- Lithium
- Sodium valproate (as semi-sodium)
- Carbamazepine
- Lamotrigine
- Other drugs used as mood stabilisers:
- Benzodiazepines
- Antipsychotic drugs

Teratogenic!
Psychiatric Pharmacy
Mood Stabilisers?
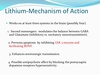
Lithium

- Lithium is the “classic” mood stabiliser
- Therapeutic drug monitoring is required to ensure lithium levels remain in the therapeutic range: 0.6- 0.8-1.2mmol/L.
- Signs and symptoms of toxicity include nausea, vomiting, diarrhoea, and ataxia (lack of voluntary coordination of muscle movements)
- Side effects are:
- Polyuria/polydipsia
- Lethargy, tremor, sedation
- Weight gain
- Blurred vision
- Hair loss
- Cardiac problems
- Long-term effects: subclinical hypothyroidism
Psychiatric Pharmacy
Mood Stabilisers?
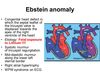
Lithium - Ebstein Anomaly

Psychiatric Pharmacy
Mood Stabilisers?
Sodium Valproate?
- An anticonvulsant medication. Indications – acute mania, acute depressive episodes and prophylaxis of BPAD
- It should be used with caution in people with:
- Decreased kidney function, history of liver disease, long-term inflammation of skin and some internal organs (systemic lupus erythematosus), diabetes
- It shouldn’t be used in people with:
- Active liver disease, personal or family history of severe liver problems, particularly if due to a medicine.
- Hereditary blood disorders called porphyrias.
- Valproate is not recommended for children and adolescents under 18 years of age, as its safety and effectiveness for treating mania have not been studied in this age group.
- Women of childbearing age.
- Most common side effects are;
- Disturbances of the gut such as diarrhoea, nausea, vomiting or abdominal pain
- Increased appetite and weight gain
- Decrease in the number of platelets in the blood (thrombocytopenia).
- Temporary hair loss -– regrowth may be curly*
- Increased alertness
- Aggression

Psychiatric Pharmacy
Mood Stabilisers
Fetal Valproate Syndrome


Psychiatric Pharmacy
Mood Stabilisers
Carbamezapine

- It is an antiepileptic drug
- It may be used under specialist supervision for the prophylaxis of bipolar disorder (manic-depressive disorder) in patients unresponsive to a combination of other prophylactic drugs
- It is used in patients with rapid-cycling manic-depressive illness (4 or more affective episodes per year)
- Side effects: Drowsiness, dizziness, ataxia, nausea, diplopia, rash (5%), agranulocytosis, leucopenia
- Neural tube defects

Psychiatric Pharmacy
Antipsychotics

- Used to treat psychosis
- Mostly used in schizophrenia and bipolar disorder
- Two types:
- 1st generation (typical) - older
- 2nd generation (atypical) - newer

Psychiatric Pharmacy
1st Generation Antipsychotics

They predominantly work by blocking dopamine D2 receptors in the brain:
- Chlorpromazine
- Levomepromazine
- Promazine
- Pericyazine
- Pipotiazine
- Fluphenazine
- Perphenazine
- Prochlorperazine
- Trifluoperazine
- Benperidol
- Haloperidol
- Flupenthixol
- Zuclopenthixol
- Pimozide
- Sulpiride

Psychiatric Pharmacy
1st Generation Antipsychotics
They are not selective for any of the four dopamine pathways in the brain and so can cause a range of side-effects (EPSE):
- parkinsonian symptoms
- dystonia (painful muscular spasms)
- akathisia (restlessness)
- tardive dyskinesia (rhythmic, involuntary movements of tongue, face, and jaw)
Hormonal side-effects (prolactin)
Temperature control (risk of hypothermia)
Antimuscarinic side effects
CVS side-effects and QT prolongation
Sudden death
Over-sedation

Psychiatric Pharmacy
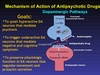
1st Generation Antipsychotics
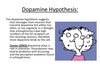
Dopamine antagonist hypothesis

- The dopamine antagonist hypothesis of antipsychotic drug action is that blocking the action of dopamine at the receptors in the mesolimbic pathway produces an effect on positive psychotic symptoms
- Blockade of dopamine receptors in the nigrostriatal pathway leads to movement disorders similar to Parkinson’s disease. The nigrostriatal pathway extends into the extrapyramidal system of the CNS these side effects are sometimes known as extrapyramidal side effects or EPSEs
- Long term blockade of the receptors in the nigrostriatal pathway can cause them to up-regulate and this can lead to tardive dyskinesia
Psychiatric Pharmacy
1st Generation Antipsychotics
Dopamine antagonist hypothesis
- Blockade of dopamine in the mesocortical pathway produces blunting of emotions and cognitive side effects known as secondary negative symptoms
- Blockade of dopamine receptors in the tuberoinfundibular pathway causes prolactin levels to rise. This can lead to amenorrhoea and galactorrhoea in women and sexual dysfunction and gynaecomastia in men
- Blockade of levels of dopamine leads to an increase of acetylcholine levels which can lead to cholinergic side effects of EPSE and hypersalivation
- Effects on the histamine receptors leads to weight gain and drowsiness
- Blockade of the alpha 1 adrenergic receptors causes hypotension and drowsiness