Skin Cancer Flashcards
(72 cards)
Session plan:

Differential diagnosis and investigation
Still consider differential diagnosis in a categorical fashion
Focuses mainly on histology and imaging in skin cancer

Melanoma-overview

- Malignant tumour arising from pigment cells ie melanocytes
- Leads to >75% of skin cancer deaths (not most common form of skin cancer, but contributes to most deaths!)
- Can arise on mucosal surfaces (e.g. oral, conjunctival, vaginal) and within uveal tract of eye (can even occur in internal organs, probs due to impaired migration during embryogenesis of melanocyte precursors.)
- Rising incidence rates observed worldwide (but mortality is stable probs due to better detection of thinner melanomas)

Melanoma: Risk Factors
Genetic factors
- Family history (CDKN2A mutations), MC1R variants
- Lightly pigmented skin
- Red hair
- DNA repair defects (e.g. xeroderma pigmentosum)
Environmental factors
- Intense intermittent sun exposure
- Chronic sun exposure
- Residence in equatorial latitudes
- Sunbeds
- Immunosuppression
Phenotypic
- People who have >100 Melanocytic nevi (moles)
- Atypical melanocytic nevi (atypical moles ie unusual asymmetrical moles)

Melanoma: Molecular Pathogenesis
Explains why some melanoma predisposition syndromes are inherited.
MAPK pathway-regulates cell proliferation, growth and migration and mutations in this pathway play a key role in melanomagenesis.
KIT mutations (can see KIT receptor in top left) are common in acral and mucosal melanomas and also melanomas that result from a high amount of chronic UV exposure.
Downstream BRAF mutations are responsible for a high number of melanomas, and to a lesser degree, NRAS mutations.

Melanoma: Molecular Pathogenesis continued (further downstream)
Further downstream, if you see in the nucelus here, CDKN2A mutations may also lead to melanoma.
CDKN2A encodes tumour suppressor called P16 and this binds to CDK 4 and 6 preventing formation of a complex. So it prevents the formation of a complex who’s role is usually to activate the cell cycle by leading to E2F release.

Melanoma: Molecular Pathogenesis
Host response to melanoma:
(this is important in terms of our therapeutic approach!)
There is a natural inhibitor we have that is called CTLA-4, and this blocks a costimulatory signal that is required for our CD8 T-cells to do their job in killing cells. Think 7 x 4=28
So we can inhibit this natural inhibitor by blocking CTLA-4 using a drug called ipilimumab.
We also have checkpoint molecules-PD-1 and PDL1 which prevent autoimmunity normally but melanoma cells can use them to signal to our immune system not to kill them. So we can use checkpoint inhibitor drugs to block these molecules.

Melanoma: Epidemiology
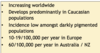
- Increasing worldwide
- Develops predominantly in Caucasian populations (high in Australia and NZ)
- Incidence low amongst darkly pigmented populations
- 10-19/100,000 per year in Europe
- 60/100,000 per year in Australia / NZ
Melanoma: Subtypes

Melanoma: Superficial Spreading
-Most common type of melanoma overall and most common type in fair-skinned individuals
Can arise in a prexisting mole or de novo

Melanoma: Superficial Spreading
What is the growth like:
Initially slow horizontal/radial growth phase limited to epidermis, here we see asymmetry, colour variation, border irregulary, increased diameter etc.
Then get vertical growth-grows upward and also downward, becomes more invasive and presents clinically with a nodule

Melanoma: Superficial Spreading
This slide shows border irregularity and colour variations
Top right can see white area-that is regression, where immune system is attacking it and is leading to formation of scar tissue.

Asymmetry, colour variation and border irregularity

Melanoma: Nodular

This is Amelanotic melanoma which is a form of melanoma in which the malignant cells have little to no pigment.
May be ulcerated and it grows rapidly

Melanoma: Nodular
What’s the growth like?
Lacks horizontal/radial phase so colour variation, border irregularity etc. are either not seen at all, or they are not as obvious.
Invades earlier as starts with vertical growth and so presents at later more advanced stage and so has worse prognosis

Not much colour variation seen, border well defined

Melanoma: Lentigo Maligna
Lentigo maligna refers to pre-invasive, slow growing, asymmetric brown to black macular (flat) lesion, with colour variation and an irregular indented border.
-When it becomes invasive, it’s termed lentigo maligna melanoma. This can take a long time and only 1 in 20 turn into this.

Melanoma: Lentigo Maligna images:
Asymmetric brown to black macules with colour variation and an irregular border

Dermoscopy-can see rhomboid structures and grey circles

Melanoma: Acral Lentiginous
Variable in how it presents, sometimes it just appears red, it can appear ulcerated as well and scaley, and non-specific. Unfortunately it can present at quite a late stage as well.

Seen in older age groups
People of African and Asian descent don’t tend to develop melanomas such as nodular melanoma, lentigo melanoma, and superficial spreading melanoma etc. so for those groups there is a disproportionate amont of this type of melanoma.

Melanoma: Nail
Can present in the nail with longitudinal pigment known as
Melanonychia (Melanonychia is brown or black pigmentation of the nail unit)

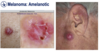
Melanoma: Amelanotic
As seen earlier, nodular melanoma, and any kind of melanoma can be amelanotic and lack any pigement
Melanoma: Self-Detection
Flag any change

Melanoma: Counselling
However these changes develop as a result of radial growth so not reliable for nodular melanoma, which is why you have to tell people E, if there is any change they should get it checked.

Differential diagnosis and investigation

Melanoma: Differential Diagnosis
Usually you can diagnose these without having to do a biopsy

Melanoma: Prognostic Factors
Thicker than 1mm-prognosis gets worse
Thin under 1mm have a 10 year survival of over 95%