soal 41 - 80 Flashcards
(32 cards)
- What abnormality is depicted on the following lateral
internal carotid artery angiogram (Figure 5.41Q.)?
A. Arteriovenous malformation
B. Primary angiitis of the GNS
C. Cavernous malformation
D. Embolic stroke
E. Moyamoya

JAWABANNYA : D
- D. Embolic strokes often exhibit an abrupt vessel cutoff on angiography, with occasional wedge-shaped regions that are devoid of blood flow and surrounding luxury perfusion (vascular blush) on late arterial phases. Occasionally an intravascular thrombus is also visualized, with slow distal antegrade flow. This lateral angiogram demonstrates a marked paucity of filling of the candelabra of the MCA, which is most consistent with embolic occlusion (Osborn DCA, pp. 383-388).
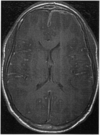
- A 35-year-old male with a history of AIDS presented with altered mental status and low-grade fever. Contrasted axial Tl-weighted MRI (Figure 5.42QJ depicts what abnormality?
A. CNS lymphoma
B. Progressive multifocal leukoencephalopathy
C. Cryptococcoma
D. Tuberculoma
E. Toxoplasmosis

JAWABANNYA : E
- E. Toxoplasmosis is the most common opportunistic infection of the CNS in AIDS patients. Toxoplasmosis usually involves the basal ganglia or gray-white junction, and is iso- to hypointense on Tl-weighted images. Toxoplasmosis exhibits prominent ring enhancement, as well as a central
enhancing region that imparts a “target” appearance, as depicted here. This target appearance is not commonly observed with cryptococcomas, tuberculomas, or lymphoma (Osborn DN, pp. 698-700).
- A 4-month-old neonate presented with macrocephaly. Axial unenhanced CT scan (Figure 5.43Q.) depicts what abnormality?
A. Pineoblastoma
B. Vein of Galen malformation
C. Sinus pericranii
D. Cavernous malformation
E. Teratoma

- B. Vein of Galen malformations (VOGM) often present
in neonates with macrocephaly, hydrocephalus, and highoutput congestive heart failure. VOGMs appear as iso- to hyperdense midline masses located posterior to the third ventricle on GT scan, often with associated hydrocephalus. Neonatal teratomas can also involve the third ventricle, however, they usually exhibit heterogenous density and intensity on GT and MRI, respectively. Germinomas rarely occur in the neonatal population (Osborn DN, pp. 320-323, 612).
- What abnormality is depicted on the following unenhanced sagittal Tl-weighted MRI (Figure 5.44QJ?
A. Pituitary adenoma
B. Rathke’s cleft cyst
C. Meningioma
D. Chordoma
E. Fibrous dysplasia

JAWABANNYA : D
- D. Chordomas arise from the clivus in approximately 35% of all cases and are typically slow-growing, lobulated extradural lesions. Calcification is often observed in chordomas; they are usually heterogenous lesions with hypointensity on Tl-weighted images and hyperintensity on T2-weigh ted images, with variable enhancement patterns.
The sella is not expanded in this example, which eliminates pituitary neoplasms from the differential, and en plaque meningiomas of the clivus are typically less lytic and invasive than chordomas. The surrounding hyperintensity (edema) of the clivus is consistent with a chordoma arising from within
the clivus itself (Osborn DN, pp. 887-890).
- An 8-week-old infant presented with a palpable scalp mass. What lesion is depicted in the following plain skull film (Figure 5.45QJ?
A. Cephalhematoma
B. Dermoid
C. Eosinophilic granuloma
D. Osteochondroma
E. Aneurysmal bone cyst

JAWABANNYA : A
- A. Cephalhematomas generally result from hemorrhage between the skull and the overlying periosteum at delivery. Cephalhematomas are initially hard and typically exhibit progressive softening as the hematoma is absorbed. Approximately 3 to 5% of all cephalhematomas exhibit calcification, usually after 6 weeks, which can require surgical resection. Cephalhematomas do not cross suture lines. The AP skull radiograph in this case illustrates a calcifying
cephalhematoma. Dermoid tumors often exhibit surrounding calcification and are located in the midline. Osteochondromas typically involve long bones or the spine, and eosinophilic granuloma often exhibits beveled nonsclerotic margins surrounding a lytic lesion involving the inner and outer tables (Osborn DN, p. 516; Wilkins, pp. 2739-2740).
- The following axial contrasted Tl-weighted MRI is located at the L3-4 disc space (Figure 5.46Q). What structure is most likely to be affected by the abnormality depicted in this MRI?
A. L3 nerve root
B. L4 nerve root
C. Both of the above
D. Neither of the above

JAWABANNYA : A
- A. Far lateral (extraforaminal) disc herniations typically compress the nerve root that is exiting at that level, as opposed to typical paracentral disc herniations, which often impinge upon the nerve root exiting at the level below. CT myelography does not typically identify far lateral disc herniations (Greenberg, p. 304).
QUESTIONS 47-51
Directions: Match the following locations and demographic information with the most likely involved primary CNS neoplasm. Letters may be used more than once or not at all.
A. Pilocytic astrocytoma
B. Schwannoma
C. Pineoblastoma
D. Germinoma
E. Meningioma
F. Choroid plexus papilloma
G. Medulloblastoma
H. Hemangioblastoma
I. None of the above
- Pineal region, 15-year-old male
- Cerebellum, 58-year-old female
- Cerebellopontine angle, 42-year-old female
- Posterior fossa, 12-year-old male
- Atrium, 8-year-old male
JAWABANNYA : D
47-D;
48-H;
49-B;
50-A;
51-F.
Germinoma accounts for approximately 66% of all germ cell tumors of the pineal region and 40% of pineal region neoplasms overall. The most common posterior fossa tumor in children is the pilocytic astrocytoma; in adults, it is the hemangioblastoma (cerebellum). Approximately 75% of all cerebellopontine angle tumors are acoustic schwannomas. Tumors of the atrium are most commonly choroid plexus papillomas in children and
meningiomas or lymphoma in adults (Osborn DN, pp. 412, 429-430, 434-436, 441, 607-608).
- What is the approximate age of the following hematoma on this noncontrasted axial CT scan (Figure 5.52Q)?
A. Hyperacute
B. Acute
C. Early subacute
D. Late subacute
E. Chronic

JAWABANNYA A
- A. The appearance of acute epidural hematomas is generally hyperdense on noncontrasted CT scans. The observance of central regions of low density in an epidural hematoma is usually secondary to the rapid accumulation of unretracted semiliquid blood clots and is known as the “swirl sign.” The lack of clear fluid-fluid levels and clot density helps eliminate subacute and chronic hematomas (Osborn DN, pp. 158-160).
- Which of the following characteristics is NOT associated with the disorder depicted in this lateral thoracic spine radiograph (Figure 5.53QJ?
A. Graniocervical instability
B. More common in young males
C. Pathologic fractures
D. HLAD15
E. Sacroiliitis

JAWABANNYA : D
- D. Ankylosing spondylitis (Marie-Strumpell disease) is an inflammatory disorder that primarily affects the spine of young males and is associated with HLA B27. Autofusion of the apophyseal joints and anterior and posterior longitudinal ligaments is commonly observed in ankylosing spondylitis. This progressive ossification is often referred to as a “bamboo” spine, which is depicted in this case. Patients with ankylosing spondylitis are prone to develop spinal fractures and craniocervical instability over time (Osborn DN, p. 849; Merritt, p. 884).
- What is the most likely histologic appearance of the neoplasm depicted in the following sagittal T2-weighted MRI (Figure 5.54Q)?
A. Small blue cells with prominent mitoses and necrosis
B. Whorls of cells with intermingled fascicular arrangements
C. Elongated cells with prominent cytoplasmic processes
and minimal pleomorphism
D. Clusters of cuboidal cells separated by a prominent
mucoid matrix
E. Lipid-containing cells within a dense network of vascular
channels

JAWABANNYA : D
- D. Myxopapillary ependymomas are located in the
conus medullaris or filum terminale and are usually
isointense to spinal cord on Tl-weighted images and isoto hyperintense on T2-weighted images, with prominent enhancement. Myxopapillary ependymomas exhibit clusters of cuboidal cells with occasional hyalinized blood vessels among a prominent mucoid matrix (Osborn DN, pp. 906-
909).
- What is depicted in this noncontrasted axial Tl-weighted MPJ (Figure 5.55Q)? The lesion did not exhibit enhancement with the administration of gadolinium.
A. Pituitary adenoma
B. Craniopharyngioma
C. Lipoma
D. Rathke’s cleft cyst
E. Histiocytosis X

JAWABANNYA : D
55. D. Rathke’s cleft cysts (RCC) result from persistence of a cleft that is found between the pars distalis and pars nervosa during the development of the pituitary gland. RCC are usually asymptomatic, and they often contain both intrasellar and suprasellar components. The appearance of RCC on MRI is variable, but they are usually hyperintense to cortex on Tl- and T2-weighted images without enhancement. RCC can be differentiated from craniopharyngiomas by the lack of calcification and from pituitary adenomas by the lack of enhancement (Osborn DN, pp. 645-646).
- What abnormality is depicted on the following axial
T2-weighted MPJ (Figure 5.56QJ?
A. Arteriovenous malformation
B. Oligodendroglioma
C. Cavernous malformation
D. Multiple sclerosis plaque
E. Hemangioblastoma

JAWABANNYA : A
- A. Arteriovenous malformations (AVMs) exhibit prominent flow voids on T2-weighted images with minimal observable intervening brain tissue and prominent enhancement. AVMs are not associated with surrounding edema unless they have recently hemorrhaged, although variable signal intensities
can be observed in and around the nidus due to the
presence of microhemorrhages of various ages and vascular thrombosis. The prominent flow voids, lack of surrounding edema, and lack of significant intranidal brain parenchyma helps distinguish AVMs from vascular tumors (Osborn DN, pp. 294-298).
- A 48-year-old female presented with headaches, nausea,and ataxia. The contrasted axial Tl-weighted MRI below(Figure 5.57Q.) depicts what abnormality?
A. Pilocytic astrocytoma
B. Choroid plexus papilloma
C. Hemangioblastoma
D. Metastatic lesion
E. Ganglioglioma

JAWABANNYA : C
57. C. Hemangioblastomas are well-circumscribed, often cystic lesions that are usually (80%) located within the cerebellum. Hemangioblastomas typically present in adults in the third to fifth decades of life, and they represent the most common primary neoplasm of the cerebellum in adults and often occur in conjunction with von Hippel-Lindau syndrome. Hemangioblastomas usually exhibit a cyst that
is hypointense on Tl-weighted images and hyperintense on T2-weighted images. The cystic component is usually associated with a mural nodule that is isointense to brain on Tlweighted images and hyperintense on T2-weighted images, with occasional flow voids. Solid hemangioblastomas often exhibit prominent enhancement, and the mural nodule of cystic lesions usually enhances as well. Choroid plexus papillomas can also occur in the fourth ventricle in adults, although they are usually solid, lobulated masses with homogenous, intense enhancement. Pilocytic astrocytomas can also exhibit prominent cyst formation with an enhancing mural nodule, although they usually occur in children and
young adults (Osborn DN, pp. 555, 574, 605-607).
- What lesion is depicted in the following AP cervical spine radiograph (Figure 5.58Q,)?
A. Eosinophilic granuloma
B. Osteoblastoma
C. Osteoid osteoma
D. Osteosarcoma
E. Osteochondroma

JAWABANNYA : E
- E. Osteochondromas are pedunculated lesions that can arise from the spinous or transverse processes of the cervical or thoracic spine. Osteochondromas are rarely symptomatic, usually present in the third to fourth decade of life, and a
cartilaginous cap that exhibits calcification covers them. Osteoblastoma is an expansile lytic mass that usually involves the neural arch, is associated with night pain, and exhibits matrix mineralization. Osteoid osteoma is similar to osteoblastoma, although smaller (< 2 cm) and usually associated with more prominent surrounding sclerosis. Osteosarcoma is an aggressive lesion associated with prominent
surrounding bony destruction/invasion and has a very
poor prognosis. The lesion depicted in this x-ray is exophytic and originates from the neural arch, which is most consistent with osteochondroma (Osborn DN, pp. 879-883).
- A 5-year-old male presented with generalized seizures and developmental delay. What abnormality is depicted on the patient’s axial T2-weighted MRI (Figure 5.59QJ?
A. Pachygyria
B. Lobar holoprosencephaly
C. Tuberous sclerosis
D. Nodular heterotopia
E. Septo-optic dysplasia

JAWABANNYA : D
- D. Nodular heterotopias are neuronal migration disorders that exhibit prominent subcortical collections of gray matter in various locations. Nodular heterotopias are often located in periventricular regions, as exhibited on the MPJ above. Nodular heterotopias resemble normal gray matter on all sequences and do not enhance. These disorders can
be differentiated from tuberous sclerosis (TS) because the cortical tubers of TS are often calcified, slightly hyperintense to cortex, and exhibit mild enhancement. The presence of a normal septum pellucidum eliminates holoprosencephaly and septo-optic dysplasia from the differential (Osborn DN, pp. 42-51).
- Which of the following imaging abnormalities is NOT
associated with neurofibromatosis type 1?
A. Optic nerve gliomas
B. Basal ganglia hamartomas
C. Thoracic meningoceles
D. Spinal schwannomas
E. Posterior vertebral body scalloping
JAWABANNYA : D
- D. Neurofibromatosis type 1 (NF-1) is associated with optic nerve gliomas, hamartomas of the basal ganglia and deep white matter, plexiform neurofibromas, spinal cord neurofibromas, kyphoscoliosis, meningoceles, intramedullary astrocytomas, and scalloping of the posterior aspects of the vertebral bodies. Spinal and cranial schwannomas are not observed in NF-1, however (Kaye and Laws, pp. 71-72; Osborn DN, pp. 73-84).
- A 21-year-old female with a prior 2-week history of
nasal congestion and frontal headaches presents with fever, leukocytosis, and confusion. Based on the patient’s axial contrasted Tl-weighted MRI (Figure 5.61QJ, what is the appropriate next step in the management of this condition?
A. Administration of broad-spectrum IV antibiotics
B. Administration of IV steroids
C. Lumbar puncture
D. Emergent surgical evacuation
E. IGU observation with repeat GT scan in 24 hours
JAWABANNYA : D
- D. The patient’s MPJ exhibits enhancement of the
mucous membranes of the frontal sinus with an adjacent subdural empyema that has spread laterally along the convexity and along the interhemispheric fissure. Subdural empyemas are associated with a high rate of cortical vein thrombosis and cerebritis, which results in their relatively high mortality (10 to 20%). Emergent surgical evacuation is indicated in almost all cases of subdural empyema, especially with the development’ of neurologic symptoms.
Approximately two-thirds of all cases of subdural empyema result from adjacent spread of infections of the frontal sinus. Nonsurgical management has been reported in asymptomatic patients with the initiation of early IV antibiotics and close IGU observation, however, most authorities advocate early surgical drainage in all cases (Greenberg, pp. 223-225; Osborn DN, pp. 684-686).
- Which of the following disorders is associated with multiple intracranial arteriovenous malformations, often involving the visual pathways and the mesencephalon?
A. Wyburn-Mason syndrome
B. Meningioangiomatosis
C. Blue rubber bleb nevus syndrome
D. Sturge-Weber syndrome
E. None of the above
JAWABANNYA : A
- A. Wyburn-Mason syndrome is a neurocutaneous syndrome that is characterized by the presence of multiple intracranial AVMs, cutaneous vascular nevi, and vascular malformations of the retina and optic nerves. The presence of multiple, discrete intracranial AVMs is extremely rare (2% of all cases), and usually occurs in the context of Wyburn- Mason syndrome or Rendu-Osler-Weber syndrome (hereditary hemorrhagic telangiectasia). Involvement of the optic
pathways and mesencephalon, however, is more characteristic of Wyburn-Mason syndrome. Meningioangiomatosis is a rare neurocutaneous disorder that is characterized by prominent fibroblastic proliferation along the meninges and Virchow-Robin spaces. Blue rubber bleb nevus syndrome is also a rare neurocutaneous disorder that is characterized
by vascular malformations of the skin, GI tract, and GNS. The CNS manifestations of blue rubber bleb nevus syndrome include the development of hemangiomas, sinus pericranii, and venous angiomas. True AVMs are not observed with this
disorder (Osborn DN, pp. 106-109, 287).
- Which of the following characteristics is NOT associated with the disorder depicted in the following GT myelogram (Figure 5.63QJ?
A. Tethered cord
B. Klippel-Feil syndrome
C. Ghiari I malformation
D. Scoliosis
E. Spina bifida

JAWABANNYA : C
- C. Diastematomyelia (split-cord malformation) is characterized by the presence of two hemicords in a single or separate dural enclosure. When the hemicords occupy different dural enclosures, they are often separated by a septum consisting of bone, fibrous, or osteocartilaginous tissue. The hemicords usually reunite into a solitary spinal cord above
and below the level of the diastematomyelia. Cutaneous stigmata often overlie the level of the split cord malformation, and it usually occurs between the levels of T9 and SI. Diastematomyelia is associated with Chiari II malformations, hemivertebrae, intersegmental laminar fusion, spina bifida, scoliosis, tethered cord, and narrowed disc spaces
(Osborn DN, pp. 811-813).
- Which of the following neurologic symptoms would a patient with the following noncontrasted GT scan (Figure 5.64Q) be most likely to exhibit?

A. Confusion and lethargy
B. Left hemiparesis
C. Right homonymous hemianopsia
D. Bilateral temporal hemianopsia
E. Receptive aphasia
JAWABANNYA : B
- B. This noncontrasted CT scan exhibits prominent
intraluminal thrombus within the right MCA, which is
known as the “hyperdense MCA sign.” This GT scan was obtained approximately 4 hours after symptom onset, which consisted of a moderate left hemiparesis and hemisensory loss (Osborn DN, pp. 344-345).
- What is the most likely etiology of the lesion demonstrated in the following lateral internal carotid angiogram (midarterial phase) (Figure 5.65QJ?
A. Trauma
B. Congenital
C. Infection
D. Dissection
E. Atherosclerosis

JAWABANNYA : C
- C. This angiogram illustrates an aneurysm along one of the distal branches of the middle cerebral artery. Aneurysms of the distal MCA are infrequent, and are usually secondary to infections of the arterial wall (mycotic aneurysm). Traumatic aneurysms that result from blunt trauma usually occur at the skull base (ICA) or along the falx (A2 segment of the ACA) (Osborn DN, pp. 271-273).
- Which of the following disorders is NOT typically associated with agenesis of the corpus callosum?
A. Holoprosencephaly
B. Aicardi syndrome
C. Dandy-Walker malformation
D. Klippel-Feil syndrome
E. Trisomy 13
JAWABANNYA : D
66. D. Agenesis of the corpus callosum can be partial
or complete and is associated with several disorders,
including Chiari II malformations, Dandy-Walker malformation, Aicardi syndrome, holoprosencephaly, heterotopias, schizencephaly, intracranial lipomas, encephaloceles, and trisomy 13, 15, and 18. Agenesis of the corpus callosum is not typically associated with Klippel-Feil syndrome (Osborn
DN, pp. 29-32).
- Which of the following characteristics is commonly
observed on plain skull films in patients with Sturge-Weber syndrome? - Thickened calvarium
- Enlarged frontal sinus
- “Tram-track” calcifications
- Elevation of the petrous temporal bone
A. 1, 2, and 3 are correct
B. 1 and 3 are correct
C. 2 and 4 are correct
D. Only 4 is correct
E. All of the above are correct
JAWABANNYA : E
- E. Skull films in patients with Sturge-Weber syndrome often exhibit prominent gyral (“tram-track”) calcifications, and secondary signs of cortical hemiatrophy (thick calvarium, elevated petrous temporal bone, enlarged frontal sinus)
(Osborn DN, pp. 98-99).
- All of the following are true about basilar impression (BI) EXCEPT?
A. Most common acquired anomaly of the craniocervical
junction
B. Often accompanied by Down’s syndrome, Klippel-Feil
syndrome, and Chiari malformation
C. Characterized by upward displacement of foramen
magnum margins (occipital bone) and cervical spine
(odontoid process) into the posterior fossa
D. McRae’s line can help make the diagnosis
E. May be seen after trauma
JAWABANNYA : A
- A. Basilar impression (BI) is characterized by upward displacement of the foramen magnum margins and cervical spine (odontoid process) into the posterior fossa. Some may refer to BI as the upward displacement of the odontoid process only. It may be associated with Down’s syndrome, Klippel-Feil syndrome, Chiari malformation, syringomyelia, rheumatoid arthritis, and trauma. It is the most common congenital (not acquired) anomaly of the craniocervical junction. McRae’s line is described as a line drawn across the foramen magnum from the tip of the clivus to opisthion (should be > 19 mm, average 35 mm). No part of the odontoid should be above this line (most accurate for BI) (Greenberg,
pp. 570-571).





