UWORLDS Flashcards
(720 cards)
where are these seen? are they all from the same disease?

NERP!
ALZHEIMERS.
A= Senile plaques in gray matter: extracellular
β-amyloid core; may cause amyloid angiopathy intracranial hemorrhage; Αβ (amyloid-β) synthesized by cleaving amyloid precursor protein (APP).
ALZHEIMERS STILL
B= Neuro brillary tangles: intracellular, hyperphosphorylated tau protein = insoluble cytoskeletal elements; number of tangles correlates with degree of dementia.
Frontotemporal dementia
C=Inclusions of hyperphosphorylated tau (round
Pick bodies; (can also see ubiquitinated TDP-43)
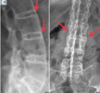
this Congenital heart defect is:
*Caused by anterosuperior displacement of the infundibular septum.
*Is the Most common cause of early childhood cyanosis.
whats the disease? what are the 4 main features?
Tetrologoy of Fallot
Pulmonary infundibular stenosis (most important determinant for prognosis)
Right ventricular hypertrophy (RVH)— boot-shaped heart on CXR
Overriding aorta
VSD (harsh systolic murmur)
Clinical syndrome characterized by acute onset respiratory failure, bilateral lung opacities “white out on CXR), LOW Pao2/Fio2, _no evidence of HF/ fluid overload.= NORMAL PCWP._
whats the diagnosis and what is characteristically seen on histo?
ARDS
Intra-alveolar hyaline membranes
what the MOA behind the AE of osteoporosis caused by corticosteroid use

man has a painless scrotal mass
no transillumination
PALPABLE WHEN STANDING BUT DISAPPEARS WHEN LAYING RECUMBANT
whats the Dx?
VARICOCELE
note: testicular cancer, spermatocele, testicular torsion DO NOT change in size when laying and although a communicating HYDROCELE (patent process vaginalis) DOES change in size it TRANSILLUMINATES SO varicocele is the only option
know how to seperate wernicke encephalopathy from korsakoff syndrome.
wernicke you get, for eaxmple. from thiamine def and it has a triad of
- ataxia
- confusion
- oculomotor dysfuntion
that resolves when given thiamine
KORSAKOFF is A COMPLICATION OF WERNICKE AND its hallmarks are PERMAMENT MEMORY LOSS AND CONFABULATION!
describe the extensive step wise tx of RA
NSAIDs, glucocorticoids,
use as a BRIDGE TO
disease-modifying agents ((DMARDS)
- methotrexate
- sulfasalazine,
- hydroxychloroquine,
- leflunomide
and when DMARDS dont work try: TNF-a inhibitors
- Etanercept -(Fusion protein (receptor for TNF-α + IgG1 Fc), produced by recombinant DNA. its a tnf decoy receptor
- Infiximab & adalimumab [Anti-TNF-α monoclonal antibody]
whats the MOA of diphendyramine of Dimenhydrinate or Meclizine?
1st gen: Reversible inhibitors of H1 histamine receptors (can cross BBB).
used for
- Allergy
- motion sickness (THIS IS DUE TO THEIR Antagonist effect at muscarinic-3 (M3) receptors)
- b (bc since they cross the BBB and have CENTRAL effects too, they cause drowsiness)

which Plasmodium class has an exoerythrocytic (dormant form (hypnozoite) in liver) form?
and how would you treat this?
is there a particular AE to look out for ?
For P vivax/ovale (not falciparum),
this how you would treat
Chloroquine (for sensitive species), which blocks Plasmodium heme polymerase;
if resistant, use mefloquine or atovaquone/ proguanil
If life-threatening, use intravenous quinidine or artesunate (test for G6PD de ciency)
AAAAND FINALLY TO ANSWER THE ACTUAL Q:
add primaquine for the exoerythrocytic (dormant form (hypnozoite) in liver)
(test for G6PD de ciency)!!!!!!
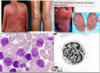
17 y/o boy
non blanching palpable purpura after taking penicilin
on biopsy what wil you see?
leukocytoclastic (cutaneous small vessel vasculitis) vasculitis!!!! (shows fragmented neutrophili nuclei + inflamed smal bv’s with Fibrinoid necrosis)
this only affects the skin and normally arises from exposure to a drug or pathogen (Hep B or C virus or penicillin, cephalsporin)
similar to what is seen in in HENOCH (leukocytoclastic angitis + IgA + C3)
which 2 vasculitis’ give you +ve p-ANCA
Microscopic Polyangitis & Churg-Strauss (eosinophilic granulomatosis with polyangitis)
Does COX-1 or COX-2 protect the GI mucosa? and how? explain which SPECIFIC PGs are made from each pathway and their diff fxs.
COX-1 (from PLTS) makes TXA2 + PGI2 and E2 where as
COX-2 (from ENDOTHELIUM) two makes PGI2
PGE2 is PROTECTIVE TO GI MUCOSA SO COX-1 IS MORE PROTECTIVE TO GI MUCOSA.
note: PGI2 is in charge of 1. dec plt. aggregation 2. vasodilation
where as COX-1 makes TXA2 which opposes (or balances) PGI2 by promoting PLT aggregation + vasoCONSTRICTION
where is the biggest O2 content difference when compared to the Aorta (that has High O2 content)?
pick one
Pulmonary Artery
IJV
Hepatic Vein
Coronary Sinus
Brachial Vein
you may want to say Pulmonary Artery BUT NO! answer is = CORONARY SINUS
the coronary sinus receives blood from the cardiac veins which are the most DEOXYgenated (O2 poor) veins in the body bc EXTRACTION/use/sucking up of O2 in the heart is the greatest out of all the veins in the body (eg: skeletal muscle) so since the CORONARY SINUS receives blood from the cardiac vein and gives it to the RA, IT IS THE PLACE THAT RECEIVES THE LEASE OXYGENATED BLOOD.
AGAIN, why not the PA?
bc it receives blood from the Coronary sinus (via the right hear) ANDDDD also from the vena cava which is MORE oxygenated than the plain ‘ol cardiac veins so since Coronary sinus JUST received SUPER SUPER DEOXY BLOOD IT IS THE PLACE THAT DIFFERS THE MOST FROM THE AORTA AS FAR AS O2 CONTENT.
main mode of transmission of HEP A?
Blood!!!!!
(IVDU, post- transfusion)
how do the levels of absorption and hence levels of Dxylose measured in blood & urine CHANGE in
- pancreatic insufficiency or removal of panc
- GI mucosal defects
- bacterial overgrowth
- NO CHange! if panc messed up it can still be absorbed bc dxylose is a MONOsaccharide (like galactose and gllucose) so they can be absorbed at proximal SI by either fac diffuusion or the SGLT1
the other 2 would DECREASE levels of dxylose seen in urine and blood
which disease has the following characteristics:
female of reproductive age
Verrucous (Libman-Sacks) Endocarditis—nonbacterial, verrucous thrombi usually on mitral or aortic valve. (DESCRIBE THE VEGETATIONS SEEN on the valve leaflets)
Associated with diffuse proliferative glomeruloneprhitis (proliferative and necrotizing lesions with crescent formation during active disease)
-what does this light microscopy look like? (looking for a buzz word here)
SLE
vegetations are seen on BOTH surfaces of valve leaflets and are composed of STERILE platelet thrombi interwined with strands of fibrin, immunecomplexes and mononuclear cells. *they are easily dislodged and can result in systemic embolization.
LM: diffuse thickennig of the glomerular capillary walls with “WIRE LOOP” structures due to subendothelial immune complex deposition”
after passing the inguinal ligament, the external iliac artery becomes the_______
Common femoral artery
What accounts for HCVs genetic instability during the replication process?
lack of 3-5’ exonuclease activity
or
lack of 5-3’ exonuclease actiivity?
they vary at sequences encoding for its 2 envelope glycoproteins
lacks 5-3’ exonuclase activity!!!!
pt with
RUQ pain (acute onset) + nausea + vomit
receiving TPN (total parenteral nutrition)
moderate leukocytosis
gallstones seen on ultrasound
why/how does TPM lead to the complication of Gallstones?
qID: 77
normally, enteral passage of fatty acids & amino acids into the duodenum–> +release of CCK–> contraction of gall bladder.
if TPN=no enteral stimuation–> no CCK released–> BILIARY STASIS–> INC RISK OF GALL STONES
side note: resection of the ileum ca also cause inc risk of gall stones due disruption of normal enterohepatic circulation of bile acids
PATIENT HAS SEPSIS AND SHOCK after pnm and after three days his hb levels drop and nasogastric suction shows bright read blood?
why?
bc THE SHOCK AND SEPSIS DECREASES BLOOD FLOW TO MUCOSA AND THIS LEADS TO “STRESS RELATED MUCOSAL INJURY!!”
LIKE HELLO…THIS IS ACUTE GASTRITIS!! EROSIONS AND THEY CAN ALSO PERFORATE.
REMEMBER WE think of nsaids and cushings and curling ulcers but SHOCK is a huge one bc our stomach NEEDS BLOOD AS A PROTECTIVE BARRIER!!!!!!!!
27-year-old primigravid woman at 18 weeks gestation comes to physician for routine prenatal examination. The uterus consistent in size with 18 week gestation. Ultrasonography shows a male fetus. The collecting system and pelvis of the left kidney is dilated and the renal cortex appears compressed.
The left and right ureters are not dilated. The right kidney appears normal. Amniotic fluid volume is normal. Which causing renal finding in this fetus ?
Incomplete recanalization of proximal ureter
a patient with a taenia infection in the intestine or (intestinal tapeworm) or Cysticercosis (eg: in muscle) would be treated with Praziquantel
BUT
neurocysticercosis is treated with….
albendazole !!!!!! for neurocysticercosis
t(8;14)—translocation of c-myc (8) and heavy-chain Ig (14)
t(14;18)—translocation of heavy-chain Ig (14) and BCL-2 (18)
t(11;14)—translocation of cyclin D1 (11) and heavy-chain Ig (14)
t(8;14)—translocation of c-myc (8) and heavy-chain Ig (14)———–Burkitt lymphoma
t(14;18)—translocation of heavy-chain Ig (14) and BCL-2 (18)———-Follicular lymphoma
t(11;14)—translocation of cyclin D1 (11) and heavy-chain Ig (14) ——–Mantle cell lymphoma