White Blood Cells and Lymph nodes, Part 1 Flashcards
(61 cards)
what is leukopenia?
how do you see leukopenia in a lab report?
what is the most affected cell?
what else may cause leukopenia?
what causes lymphopenia?
decrease in number of circulating white blood cells
WBC = less than 4,000
neutrophils
lymphopenia
occurs due to whole body radiation, imunodeficiency (HIV, DiGeorge), corticosteroids
Neutropenia & Agranulocytosis
what can cause neutropenia? what causes these?
1) Inadequate or ineffective granulopoeisis
* Suppression of hematopoeitic stem cells: Aplastic anemia, and marrow infiltration (tumors and granulomatous dis)
* Suppression of committed granulocytic precursors: due to drugs (most common cause)
* Diseases associated with ineffective hematopoeisis: Megaloblastic anemia, MDS
* Rare congenital diseases: kostmann’s syndrome
2) Accelerated removal or destruction of neutrophils
* Immunologically mediated: SLE
* Splenomegaly: splenic sequestration
* Increased peripheral utilization: bacterial, fungal, rickettsia
what is neutropenia in a lab report?
what is mild neutropenia?
what is moderate neutropenia?
what is severe neutropenia?
what is agranylocytosis?
less than 1500
1000-1500
500-1000
less than 500
less than 100
how do you confirm neutropenia and agranulocytosis?
total WBC = reduced
peripheral blood smear = neutropenia
absolut neutrophil count = reduced
bone marrow: hypocellular if drug induced
hypercellular when there is increased peripheral destruction of neutrophils
what is noticible in this picture?

absence of neutrophils
what can be noticed here?

hypocellularity of the bone marrow
when do you know there is a serious infection?
what are some examples of secondary infections to agranulocytosis?
what is the treatment for these conditions
when neutrophil count drops below 500
infections:
1) ulcerating necrotizing lesions of : gingiva, floor of mouth, buccal mucosa
2) severe life threatening infections: lungs, kidney deep fungal infections: Candida and Aspergillus
Treatment:
granulocytic transfusions using recombinant granulocyte growth factors: G- CSF, GM- CSF
what is this?

Candida albicans of oral mucosa
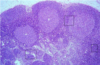
what are 2 types of proliferative disorders that are reactive (or inflammatory)?
1) leukocytosis
2) lymphadenitis
what are the 2 division types of lymphadenitis?
1) acute non-specific lymphadenitis
2) chronic non-specific lymphadenitis
what is 1 type of proliferative disorder that is neoplastic?
1) Neoplastic Proliferation of White cells
what is the normal white cell count for adults?
what is the normal range for these in adults:
neutrophils
lymphocytes
monocytes
eosinophils
basophils
4000-11000
neutrophils: 40-70%
lymphocytes: 20-40%
monocytes: 1-8%
eosinophils: 1-6%
basophils: 1%
what are the 2 special types of leukocytosis?
1) leukemoid reaction
2) Leukoerythroblastic reaction
what is a leukemoid reaction?
what appears in a peripheral smear with this condition?
when could the white count be higher?
some inflammatory states or chronic infections cause the total white cell count to be elevated (WBC more than 50000)
immature granulocytes
chronic myelogenous leukemia (CML)
how do you differentiate between CML and leukemoid reaction?
unsing a LAP score (leukocyte alkaline phosphatase):
- increased in Leukemoid reaction
- low in chronic myeloid leukemia (CML)
what is a left shift?

red cell clumping due to preparation, not pathological
what is this?

‘band’ neutrophils in peripheral smear
what is this?

Neutrophil metamyelocyte in peripheral smear
what is Leukoerythroblastic reaction?
what is its pathogenesis?
what do you see in a peripheral smear?
- immature granulocytes and eryhtroid precursors enter peripheral blood
- bone marrow infiltration (amyloidosis, Gaucher’s,
leukemias, metastatic cancers)
- marrow fibrosis occurs
you see immature granulocytes, and nucleated red cells
what do you see in this peripheral blood smear?

Leukoerythroblastic reaction
note: numerous nucleated red cells (red arrow and immature granulocytes-white cells (green arrow)
what do you see in this peripheral smear?

Leukoerythroblastic reaction: blood smear showing neutrophils, immature granulocytes, lymphocytes, and nucleated red cell.
where do you see toxic granulations?
how do you identify them?
in severe infections with sepsis
neutrophils contain numerous dark purple granules
what is this?

toxic granulation
what is the first thing you think when you hear lymphocytosis?
viral infection