Chapter 13 - Blood vessels Flashcards
Review:
What is the intima?
What is the media?
What is the adventitia?
How are they supplied?
-
Intima
- Single layer of endothelial cells with little subendothelial CT
- Supplied by the lumen
- Separated from media by the internal elastic lamina
-
Media
- Smooth muscle
- Inner layers: lumen
- Outer layers: small arterioles (vasa vasorum)
-
Adventitia
- CT, Nerves, and Vasa Vasorum
Review
Difference between large, medium, and small arteries?
- Large (elastic arteries)
- Media = rich in elastic fibers that alternate with layers of smooth muscle
- Medium (muscular arteries)
- Media = mostly smooth muscle
- Small (less than 2mm)
- Structurally similar to medium arteries
- Found within tissue and organs
Review still:
Arterioles:
Composition?
Importance?
Capillaries:
Composition?
Importance?
- Arterioles
- Small amount of smooth muscle
- NO elastic lamina
- *Principle sites of BF resistance*
- Capillaries
- Endotheilal lining but NO media
- BF slows dramatically here obbbbbviously for nutrient exchange
Review:
Where does blood flow after capillaries? What is important about these?
Veins in comparison to arteries?
Composition of lymphatics?
- Postcapillary venules (after cap)
- Site of inflammation induced leakage
- Veins
- Large lumens and walls (less organized than art.)
- Contains 2/3 of all blood
- Lymphatics
- Thin-walled, endotheium lined channels
- Drain intersitial fluid and inflammatory cells
How are endothelial cells identified immunohistochemically?
Endothelial cells identified by:
- PECAM-1 (CD31)
- CD34
- vWF
Functions of endothelial cells?
Endothelial cell function:
- Maintenance of permeability barrier
- Elaboration of compounds that control coagulation
- Produce ECM proteins for healing/angiogenesis
- Production of vasoconstrictors (endothelin/angiotensin)
- Production of vasodilators (NO/prostacyclin)
- Important mediators of inflammation
- Produce IL-1/6/8
- Express VCAM-1, ICAMS, E/P selectin
- Produce growth factors
What is endothelial dysfunction associated with?
Endothelial dysfunction:
- Abnormal thrombus formation
- Atherosclerosis
- Vascular lesions of hypertension
Functions of vascular smooth muscle cells?
Vascular smooth muscle cells:
- Vasodilation/constriction in response to mediators
- Synthesis extracellular basement membrane proteins
- Collagen, elastin, and proteoglycan
- They can also proliferate and be migratory
- In response to cytokines (IL-1, IFN)
- In response to GF (PDGF, endothelin-1, and FGF)
What layer of the artery thickens in response to vessel injury?
The intima
What is the pathology of intimal thickening in response to vessel injury?
Pathology
- Endothelial cells lose the ability to contract but they proliferate and produce ECM proteins, creating what is known as the neointima*
- If chronic - associated with atherosclerosis
Arteriosclerosis:
Generic term for?
What are the 3 variations?
Arteriosclerosis:
- Arterial wall thickening and the loss of wall elasticity
3 variations:
- Monckeberg medial calcific sclerosis
- Arteriolosclerosis
- Atherosclerosis
What is monckeberg medial calcific sclerosis?
Characterized by excessive Ca++ deposits in muscular arteries (50+ yo) that are usually benign because the deposits do not cause obstruction
What is arteriolosclerosis?
Involves arterioles and small arteries
Hyaline and hyperplastic forms occur and are associated with thickening of the vessel walls and obstruction of the lumen
What is atherosclerosis characterized by?
Characterized by intimal lesions known as atheromas or atheromatous fibrofatty plaques
(they may obstruct the lumen and weaken the media)
What is this an example of?

This is Monckeberg medial calcific sclerosis with the collection of calcium deposits (arrows) in the media of small muscular arteries
Where do atherosclerotic lesions primarily develop?
Atherosclerotic symptomatic disease most often involves the arteries supplying what organs?
- Lesions develop in:
- Elastic arteries (aorta, carotid, and iliac)
- Large/medium muscular arteries (coronary/popliteal)
- Symptomatic disease involves arteries supplying:
- Heart
- Brain
- Kidneys
- Lower extremities
Major outcomes of atherosclerosis?
Atherosclerosis major outcomes:
- MI
- Stroke
- Aortic aneurysms
- Peripheral vascular disease
Earliest lesion of atherosclerosis
Earliest lesion:
- Fatty streaks in the intima
- Lipid filled macrophages (foam cells)
- Not raised so no disturbance in BF
Atherosclerotic plaques typically have what 3 principal components?
- Cells
- Smooth muscle, macrophages, and lymphocytes
- ECM proteins
- Collagen, elastic fibers, and proteoglycan
- Intra/Extracellular Lipid
- Cholesterol clefts are common
Top risk factors for CVD?
- Hyperlipidemia
- Hypertension
- Cig smoking (oops)
- Diabetes
- Advanced age
Response to injury hypothesis implies?
Implies that atherosclerosis is a chronic inflammatory response of the artery wall initiated by injury to the endothelium
Lesion progression of atherosclerosis is sustained by?
Sustained by interactions between
- lipoproteins
- Macrophages
- T cells
- Smooth muscle cells
Steps in lesion development?
- Chronic injury
- Accumulation of lipoproteins (mostly LDL)
- Increased adhesion of monocytes/leukocytes to endo.
- Adhesion of platelets
- Release of factors that induce smooth muscle migration
- Smooth muscle proliferation
- Elaboration of extracellular matrix proteins
What is C-reactive protein?
CRP = one of the cheapest and most sensitive predictors of the risk of MI, stroke, peripheral arterial disease, and sudden cardiac death
How can the endothelium become damaged to create plaques?
Endothelial damage:
- May be associated with infection
- Initiated by normal hemodynamic disturbances
- Eg: at branch points
- Hypercholesterolemia
Inflammatory role associated with plaque formation?
- Increases expression of adhesion molecules by endothelial cells
- Allows for infiltration of inflammatory cells to intima
- This is initially protective until T cells become activated
- Secrete proinflammatory cytokines that induce smooth muscle migration/proliferation
What are the major lipids in atheromatous plaques?
Correlation between the severity of atherosclerosis and?
- Major lipids
- Plasma derived cholesterol and cholesterol esters
- Correlation of severity with:
- High levels of plasma cholesterol or LDL
Smooth muscle cells convert the fatty streak into what?
Catastrophic evens are associated with what aggregation?
- Smooth muscle cells convert fatty streak to
- Fibrofatty atheroma
- Catastrophic events are associated with platelet aggregation over the plaque
- This is followed by eventual disruption of the fibrous cap

When does atherosclerotic coronary artery disease begin?
Childhood (modification should begin then)
Hyptertensive vascular disease BP:
Normal?
Prehypertensive?
Stage 1 hypertension?
Stage 2 hypertension?
- Normal
- <120/80
- Prehypertension
- 120-129/80-89
- Stage 1
- 140-159/90-99
- Stage 2
- >160/100
Types of hypertension?
- Essential hypertension
- idiopathic and some develop potentially fatal BP
- Secondary
- Underlying renal or adrenal disease
What relationship is altered in arterial hypertension?
The relationship between cardiac output and TPR
( BP = CO x TPR )
What is cardiac output dependent upon?
Where is TPR determined?
- CO
- Blood Vol influenced by Na+ homeostasis
- TPR
- Determined at the arterioles
Role of the kidney in BP regulation?
- Renin converts A to AI which is then converted to AII bye ACE
- AII increases BP by increasing peripheral resistance and increasing the blood volume by increasing Na+ resorption
- Kidney also produces antihypertensive substances (PG/NO)
- Counterbalances AII
- Natriuretic Factors inhibit Na+ resorption and induce vasodilation
What three pathological dysfunctions alter Renin secretion?
- ( - ) Fibromuscular dysplasia
- Genetic disorder
- ( + ) Renal artery stenosis
- Acquired Disorder
- ( + ) Renin-secreting tumor
- Acquired Disorder
What two things alter angiotensin (A) secretion?
- ( + ) Oral contraceptives
- Acquired
- ( - ) Angiotensinogen Variants
- Genetic disorder
What three pathological dysfunctions alter Na+ reabsorption?
- ALL ( - ) Genetic Disorders
- Liddle Syndrome
- Pseudohypoaldosteronism
- Gitelman syndrome
Hyptertension is associated with what two forms of arteriolosclerosis?
Hyaline and Hyperplastic
What is hyaline arteriolosclerosis?
- Lesion consists of a homogeneous hyaline thickening of the wall with eventual narrowing of the lumen
- These reflect the leakage of plasma components across the endothelium and excessive ECM production by smooth muscle secondary to the hemodynamic stress associated with hypertension
- Contribute to hypertension related renal failure
What is hyperplastic ateriolosclerosis?
- Associated with severe hypertension
- Concentric, laminated thickening of the arterioles composed of smooth muscle and basement membrane components
- May become necrotic and infiltrated with fibrin
- Also common in the kidney
What is this?

Hyperplastic arteriolosclerosis
(Concentric - looks like an onion )
What is this?

Hyaline Arteriolosclerosis
What is a TIA?
Characterization of a TIA?
- TIA
- Mini stroke that lasts less than 24 hours
- Characterized by focal neurological defects that resolve within 24 hours
Difference between an aneurysm and a false aneurysm?
What is a Dissection?
- Aneurysm
- Abnormal dilation of a vascular wall
- False aneurysm
- Breach in the vascular wall leading to an extravascular hematoma
- Dissection
- Blood enters the artery wall and travels for a distance
Note* aortic aneurysm/dissections are clinically the most important
Despite that the picture kindddda tells you.. what are these from left to right (1-4)?

- True aneurysm (saccular)
- True aneurysm (fusiform)
- False aneurysm
- Dissection
Saccular versus fusiform aneurysms?
- Saccular
- Spherical and involve only a portion of the vessel wall
- Usually contain a thrombus
- 5-20 cm in diameter
- Fusiform
- Vary in diameter/length
- May involve the entire segment
Major cause and location of abdominal aortic aneurysms?
Atherosclerosis usually right below the renal arteries and above the bifurcation
What predisposes to aneurysms and dissections?
- Genetic defects in CT structure and/or assembly
- Example: Marfan syndrome
- Overactive metalloproteinases (w/ chronic inflammation) may degrade CT and weaken the vessel wall
Clinical course of the abdominal aortic aneurysm?
- May rupture with massive hemorrhage, obstruction of lumen, obstruction of neighboring vessels/organs, and/or emolism
- May present as a mass simulating a tumor
- Most expand until they rupture
What occurs in syphilitic aneurysms?
- This occurs in tertiary syphilis as an aortic obliterative endarteritis
- Inflammation and fibrosis weaken the media
What is aortic dissection characterized by?
- Dissection of blood between and along the laminar planes of the media
- Often rupture outward causing a massive hemorrhage
(90% in men btwn 40-60yo with HT, others due to CT abnormalities or as a result of arterial cannulation)
Most common pathologic abnormality of aortic dissection
- Cystic medial degeneration
- Characterized by fragmentation of the elastic tissue and separation of the elastic/fibromuscular element by clefts
- Frequently occurs in Marfan syndrome
What is this?

Giant cell arteritis:
Granulomas in the media (black arrows)
Lumen is almost entirely occluded (yellow arrow)
What is this?
What is the black arrow pointing at in figure A? Figure B?
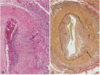
Giant cell arteritis
A: degenerated internal elastic lamina in active arteritis
B: focal destruction of internal elastic lamina and intimal thickening of long-standing/healed arteritis
What is this?

PAN: Polyarteritis Nodosa
Shows inflammation, necrosis, and fibrosis (and karyorrhexis as a bonus if you remember nuclear fragmentation)
What disease is this?

Takayasu arteritis
A: narrowing of aortic arch branches
C: destruction of the media w/ mononuclear infiltrates, giant cells, and fibrosis
What disease are you likely to find this in?
(THIS ONES A TOUGHY!)
Henoch-Schonlein purpura:
IgA deposits limited to the mesangium and thus the capillary walls are not outlined
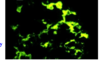
Which is P-ANCA? C-ANCA?
What Diseases are each associated with?

P-ANCA: on the left; associated with Microscopic Polyangiitis
C-ANCA: center and right; associated with Wegener’s