PNS/Muscle Flashcards
PNS/MUSCLE I
What is happening to the nerve in the image?

Segmental demyelination
•Schwann cell dysfunction or myelin sheath damage
•No primary abnormality of axon
•Not all Schwann cells along length of axon involved
•Degenerating myelin engulfed by Schwann cells later by macrophages
•Denuded axon induces remyelination by stimulating Schwann cell stem cell proliferation
What pathology do you see in this image? Explain.

- Segmental demyelination: Axon in the top right should be myelinated
- Same size as the two heavily myelinated axons in the bottom of the image
What is occuring in this axon?

Repeated bouts of demyelination and remyelination results in multiple layers of Schwann cells surrounding axon giving it an onion bulb appearance – onion bulb neuropathy
What is occuring? Primary and secondary findings?

Axonal degeneration
•Primary destruction of axon
•Secondary degeneration of myelin sheath
•May be focal destruction or generalized insult
•Response to transection or focal lesion
•Wallerian degeneration
Wallerian degeneration comes from focal damage and the axon may break down within a single day. Chromolysis (loss of nissl bodies) and perikaryon swelling occurs and the schwann cell begins to digest myelin. Denervated muscle cells atrophy
What can you see in this image?

Top middle clustering:
Suggestive of resprouting of axons (multiple)
The thinness of the myelin implies that this is a recent event
What are these?

Regeneration cluster – Growth cone
- Multiple filipodia/lamellapodia lead small caliber axons
- These are closely aggregated and thinly myelinated
- They typically follow the cord of Schwann cells
- Slow axonal transport: grow only 1mm/day
- Limit = slow rate of transport from synthetic activity in the nucleus
What disease is this associated with?

Guillain-Barre Syndrome
- Can see inflammation (at the top) of the peripheral nerve with perivenular and endoneural infiltration of lymphocytes, macrophages and a few plasma cells
- Commonly motor roots of spinal and cranial nerves
- Macrophages penetrate at the nodes and peel away the myelin layers
What disease is this a typical stain for?

Leprosy: cellular immune response determines which morphology
- Lepromatous leprosy - Schwann cell invaded by bacteria causes segmental demyelination/remyelination, loss of both M/UM fibers, and endoneurial fibrosis and thickening of perineural sheaths
- ——–symmetric polyneuropathy with primarily sensory loss in cooler extremities
- Tuberculoid leprosy - active cell-mediated response - nodular granulomatous inflammation in dermis injuring cutaneous nerves, perineural and endoneurial fibrosis
- ——more localized nerve damage of axons, Schwann cells, perineural and endoneural layers
What is this image associated with? What is this stain for?

This is also leprosy
This stain is for bacterial cells in the endoneurium. Acid fast positive lepra bacilli
What is this?

Diptheria - Corynebacterium diphtheriae
- Gram positive rod with clubbed ends
- Exotoxin initially effects peripheral nerve and causes paresthesias and weakness
- Characteristic early loss of proprioception and vibratory sensation
- Toxin enters sensory ganglia due to incomplete blood-nerve barrier
- Demyelination extends into adjacent anterior and posterior roots
- mixed sensorimotor nerves
- A toxin blocks protein synthesis by adding ADP-ribose to elongation factor 2
This one is tricky: what is going on here?

Adult Onset Diabetic Neuropathy
- Arrowheads only
- large axon with a thin sheath indicating an ongoing process
- Arrow
- vascular changes here with duplication of the basement membrane
- Mechanism is thought to be advanced glycation end products
- Most commonly ascending distal symmetric sensorimotor neuropathy
- Loss of small M and UM fibers
- Large fibers also affected - those remaining have less myelin
- Endoneurial arterioles show diabetic vascular thickening
PNS/MUSCLE II
What disease is this image associated with?

Charcot-Marie-Tooth 1
- AD inheritance in childhood/early adulthood
- Repeated segmental demyelination –> onion bulbing
- Hypertrophy of individual peripheral nerves
- May have palpable nerve enlargement
- Distal leg weakness and progressive muscular atrophy of the calf (peroneal muscular atrophy)
- Pes cavus
What is this? What be happenin?

This is the result of axonal degeneration and denervation
Myofibers that lose their innervation become angular and shrink. At an extreme stage of atrophy virtually all the sarcoplasm is lost and the myofiber is reduced to a cluster of nuclei. No myonecrosis
What is happening in this image? What disease is it associated with?

This is atrophy below the knee (peroneal muscular atrophy) with characteristic foot seen in Charcot-Marie Tooth
What is occuring in the image?
Result?

Segmental myocyte degeneration
• Destruction of a portion of the length of myocyte
•Release of creatine kinase
• Results in phagocytosis
•Activation of satellite cells in regeneration attempt
•Continuity of original myofiber may be restored
• May also lead to deposition of collagen and fatty infiltration in time if sufficient necrosis occurs or if repeated bouts of necrosis
What is occuring to the cell at the arrow?

Muscle fiber splitting
• Invagination of membrane along large fibers, with apparent longitudinal splitting of fibers
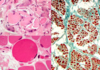
All three of these images are related to the same disease: what is that disease?

Dermatomyositis
Perifascicular atrophy with small muscle cells at teh edges of the fasicle with immune inflammatory accumulations
Key: small vessel damage is very important in this disease and can see that in the bottom picture
What is this?

Inclusion body myositis
- Most common inflammatory myopathy in persons 65+
- Rimmed vacuoles with basophilic granules at the periphery
- Vacuolated fibers stain with congo red
- Inflammatory infiltrate similar to polymyositis but also share some features of neurodegenerative origin
Additional image with examples attached to also show variability of inflammation

What disease is this? What do you see in the image?

Duchenne MD:
- Different states of degeneration and regeneration (more basophilic cytoplasm).
- Eventual loss and replacement with fat at CT
- Proliferation of endomysial CT
- Bottom image: see enlargement of central cell = this is the first sign of change
- Large image: Increased CT and change in myocyte size
What is this?

Myotonic Dystrophy
- Can see a subsarcolemmal band of cytoplasm around the muscle cells (light pink stain)
- Multiple internal nuclei
- Atrophy of T1 fibers relative to T2
What disease is this? How do you know immediately?

Myotonic dystrophy
Can see that myofibrils are oriented in a circular manner as well as sarcoplasmic masses and visible sarcolemmal band of cytoplasm in the unstained EM
What are dis?

Central core disease
- Ryanodine receptor 1 mutation
- Cytoplasmic cores are lightly eosinophilic and distinct
- Decreased mitochondria
- Not regenerating here
Cool staining colors! Wahoo! What is this? What can you see?

Nemaline myopathy
- Affects Type I fibers
- Subsarcolemmal spindle shaped particles
- Dense material that is the same as Z-band (alpha actinin)
- MORE PRETTY COLORS FOR YOUUUU!

What is this?

Centronuclear myopathy
- nuclei in the center of the cells
- More common in T1
- small cell diameter: fetal like arrangement
What is this?

Spinal muscular atrophy
- Left image
- This is group atrophy in adult with angulated atrophic cells
- Right image (SMA)
- Disease of childhood
- Panfascicular atrophy without angulated cells
- Rounded cells and a few hypertrophic cells
- Due to loss of motor neuron
What is this? (hard - vague?)

Lipid myopathy
•Carnitine palmitoyltransferase II deficiency
•Carnitine transport system abnormalities or mitochondrial dehydrogenase deficiencies blocks fatty acid oxidation
•Accumulation of lipid droplets in myocytes
•vacuoles primarily Type 1 fibers
What disease is this?

McArdle Disease
- Myophosphorylase deficiency
- Glycogen storage disease
- PAS+
- (in comparison to Pompe’s where there is acid maltase deficiency with lysosomal accumulation of glycogen)
What disease is this association? What do you see in each of the pictures?

Mitochondrial myopathies
- Top Left
- Visible ragged red fibers
- Bottom Left
- accumulation with abnormal mitochondria stained purple
- Bottom right
- abnormal crystalline formation within the mitochondria