10/19- Pathology Review Flashcards
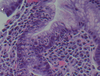
What is seen here?

Viral esophagitis (typical of herpes):
- Margination of chromatin
- Nuclear molding
- Multinucleate
Also ground glass appearance of nuclei and necroinflammatory debris (ulcer)
What is seen here?

Viral esophagitis (typical of herpes):
- Margination of chromatin
- Nuclear molding
- Multinucleate
Also ground glass appearance of nuclei
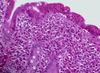
What is seen here?

Fungal esophagitis- Candida
- Pseudohyphae in squamous cells
- Yeast forms
Recall: Candida is part of flora in oral cavity; if just sitting in lumen, it’s probably contaminant. Must diagnose by seeing within tissue
What is seen here?

Barrett’s esophagitis (intestinal metaplasia)
- Can see goblet cells
- This is at the GEJ
- Predisposition to developing adenocarcinoma
What is seen here?

Adenocarcinoma
- Cells with dark nuclei with different shapes and sizes
- Gland formation
What is seen here?

Squamous cell carcinoma
- May be hard to differentiate adenocarcinoma and squamous sometimes, but as general rule, if you don’t have glands and do have tight junctions, think squamous
What is seen here?

Stomach (body/oxyntic) mucosa
What is seen here? (what cells)?

Stomach (body/oxyntic) mucosa
- Pink = parietal cells; secrete acid
- Blue = chief cells; secrete pepsinogen
What is seen here?

Antral (cardiac mucosa)
What is seen here?

Iron pill ischemia
- Can see inflammatory cells
- Brown material in surface of epithelium
What is seen here?

Iron pill ischemia
- Has ulcerated
- Brown refractile material from iron pill
What is seen here?

Autoimmune gastritis; chronic active gastritis
- Lymphoid follicles
- Think H pylori until proven otherwise?
What is seen here?
Autoimmune gastritis; chronic active gastritis
- Neutrophils infiltrating epithelial cells
- Associated with H. pylori
What is seen here?

H. pylori spiral bacilli
- Chronic active carditis is associated with H. pylori
What is seen here?

Stomach with intestinal metaplasia
- Goblet cells
What is seen here?

Adenocarcinoma: Intestinal (bulky) type
- Glands present of different size and shape
What is seen here?

Adenocarcinoma: Intestinal (bulky) type
- Many mitotic figures
- Enlarged nuclei of different size and shape
What is seen here?

Adenocarcinoma: poorly differentiated type
- Signet ring cells: mucin filling pushing nuclei to periphery
What is seen here?

Small intestine mucosa
- Villi and crypts (V:C ratio should be 3-5:1)
- Paneth cells in base of crypts (more eosinophilic)
- Can also see muscularis mucosa layer on the right
What is seen here?

Duodenum (normal histology)
What is seen here?

Ischemic colitis
What is seen here?
Celiac disease
- Increased chronic inflammatory cells in lamina propria
- Many lymphocytes in the epithelial cells
- Blunted villi
What is seen here?

Whipple’s disease
- Expanded villus
- Huge macrophages
What is seen here?

Whipple’s disease
- Bacteria overload
- Mostly MAC (mycobacterium avium ); typically diagnose with acid-fast stain
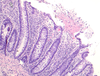
What is seen here?

- There are NO villi in colon!
- Crypts here look like test tubes in a rack and they reach the muscularis mucosa
- Submucosa layer also seen here?

What is seen here?

Normal colonic histology
- Equally spaced crypts
- Separated by vessels
What is seen here?
Pseudomembranous colitis
- “Volcano eruption” of neutrophils and dead cells
- Increased chronic inflammatory cells in lamina propria

Important: compare Crohn’s disease and Ulcerative colitis in terms of:
- Location (layers and along length)
- Features
Crohn’s disease
- Skip lesions
- Most common location = terminal ileum
- Transmural inflammation, ulcerations, fissures
Ulcerative colitis:
- Does not reach muscularis mucosa
- Always have rectum involvement!
- Continuous involvement as it moves proximally
- Psuedopolyp, ulcer

What is seen here?

Crohn’s disease
- Increased chronic inflammatory cells in lamina propria; crypts no longer equally spaced
- Granuloma
What is seen here?

Diverticulum/diverticulosis (diverticulitis if inflamed)
- Mucosa pushed down; can go down through muscularis propria and serosa if severe
- From mucosal side, you see holes
What is seen here?

Polyp
- Can see normal layers of intestinal wall
What is seen here?

Polyp: tubular adenoma
- Base of the polyp is on the bottom right
- Normal colonic mucosa (pedunculated tubular adenoma) on the bottom right; the rest of the crypts are darker
What is seen here?

Villous adenoma
- If less than 25% has villous architecture, you still call it tubular
- If more than 75% has villous architecture, it’s “villous”, but anything in between (25-75%) is “tubulovillous)
What is seen here?

Adenocarcinoma of colon
What is seen here?

Colon adenocarcinoma
- Glands with necrotic material inside
- Multinucleate cells
- Many mitotic figures
What is seen here?

Chronic cholecystitis (gallstones in gallbladder)
- Fibrotic (inside appears like outside; abnormal)
- Stones press on mucosa -> atrophy
What is seen here?

Adenocarcinoma involving gallbladder
- Typically seen in older women
- Just the thickened wall piece with whitish color (pretty localized)
What is seen here?

Normal appendix
- Many lymphoid aggregates and follicles (fewer as you age)

What is seen here?

Acute appendicitis
- Focal ulceration of mucosa
- Collection of neutrophils
- To diagnose, must have neutrophils in muscularis propria
What is seen here?

Acute appendicitis
- Neutrophils in muscularis propria (necessary to diagnose acute appendicitis)
What is seen here?

Serosa/mesothelial cells (benign to reactive transition)
- Mesothelial cells are flat at rest
- Become round and columnar when irritated
What is seen here?

Acute serositis, marked
- Layers of neutrophils
- Reactive mesothelial cells (if chronic, can proliferate and become columnar, but this reactivity happens first)
