GI Portion Flashcards
gastroesophageal reflux disease
what is this?
population common in?
percent in US?
5 complications it can lead to
most common dxs of esophagous 15-20% US, common in pregnancy

transient relaxation of lower esophageal spincter LES leading to gastric acid reflux that causees damange to esophagus and spincter and can lead to:
1. esphagitits- 50% will get this!!!
2. esophageal stricutre
3. barrettes esophagous
4. esophageal adenocarcinoma
- hiatial hernia
-
GERD
what are 6 sxs?
1 thing to keep in mind about sxs?
- heartburn, restrosternal and postprandial
substernal pain/discomfort most commong 30-60 minutes after a meal
worsens when laying down or recumbant
- regurgitation (vomit burp)
spontaneous reflux of sour bitter gastric contents in mouth
- dysphagia (discomfort)
cough at night from acid asipiraiton
- reccurent pneumonia
- sxs temp relieved with antacids
- can radiate to arm/jaw
***keep in mind sxs don’t correlate with dxs progression so can’t tell how much damage has been done**
what is the pathway for txing GERD?
6
- lifestyle adjustments
- OTC antacids-2 weeks
- H2 receptor antagonists
- Proton pump inhibitors
**if these fail EDG**
- prokinetics
- surgical

GERD
3 dx options
6 reasons of when it is not appopropriate to use the first line dx
- empirically first line unless (below)
- esphagogastroduodenoscopy(EGD) if high risk or tx has failed
a. over 50
b. weight loss
c. melena
d. odynophagia pain with eating
e. heavy alcohol or tabacco
f. non repsonsive to tx - modified/full barium swallow
what are the lifestyle changes a patient should make to relieve sxs of GERD?
5
- avoid eating 2-3 hours before bed
2. elevate head of bed
3. loose weight
- avoid acidic food, chocolate, peppermint, ETOH, coffee
- stop smoking
why is it important to treat GERD?
prevent cancer aka barrette esophagus because the damange from acid makes this more likely to occur
what is the emergency cocktail you give someone in the ED for heart burn?
- benadryl
- lidocaine
- maalox
what is the most common cause of esophagitits?
GERD, 50% of patients with GERD have esophagitits
esophagitits
what is this?
5 general causes?
4 sxs
inflammation of the esophagus, esp in immunocomprimised
- viral
- bacterial
- paraistic
- abx induced
- radiation or chest cancers
sxs;
- odyniaphagia
- dysphagia
- substernal chest pain
- oral thursh
esophagitis
herpes liabilis (HSV)
3 SXS?
2 DX?
1 TX
N/V/ chills
herpetic vesicles on nose/lips
dx:
1. endoscopy showing small vesicles or superficial lesions
2. culture esophageal lesions
TX:
ACYCLOVIR 7-21 DAYS!!!
ESOPHAGITIS
VARICELLA-ZOSTER
1 dx?
tx?
N/V fever chils
DX:
endoscopy: vesicles or confluent ulcers
Tx:
- usually resolve spontaneously but can cause necrotizing esophagitits
- ACYCLOVIR!!!!
esophagitis
CMV
who does this occur in?
characteristics of ulcer? 2
3 sxs?
1 tx?
only occurs in immunocomprimised patients
CREEPING ULCER or can be GIANT ULCER
sxs:
odyniaphagia
persistent CP
hematememis
Tx:
IV GANCICLOVIR
esophagitis
candidia
who does it occur in?
3 complications?
1 dx?
1 tx?
occurs in immunocomprimised host
can cause complications:
- bleeding
- perforation
- stricture
dx:
endoscopy: small yellowwhite raised plaques
tx:
oral or IV fluconazole!!
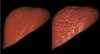
barrett’s esophagus

how does this occur? what hcanges?
what are they at increased risk for? how much?
metaplastic changes in which the stratified squamous** is replaced by the **columnar epithelium that is typically found in the duodenum….extens poximally from LES from repeated exposure to acid esp with GERD (thats why the cells change to this type because its the same exposure the duodenum gets)
increases risk for adenocarcinoma 5-10%
this change increases risk for neoplastic changes/cancer 40-100 times greater than general public
barettes esophagus

2 dx rules?
3 tx?
DX:
EDG every 2 years with bx to check for neoplastic changes
if there is high risk dysplasia, consider surgrical resection
TX:
**more txing symtpoms unless surgical intervention**
- antacids
- H2 blockers OTCs
- PPIs
esophageal cancer
what are the two types?
frequency?
prognisis?
who is more common?
types:
- adenocarcinoma
- squamous cell carcinoma
prognosis typicaly poor, 5 year survival 10-13%
both appeare with equal frequency
males more common than females
esophageal cancer:
adenocarcinoma
where do you find this?
4 most important RF?
2 protective

distal esophagus
RF:
- reflux over 20 years
- Barrettes esophagus-almost all cases
- obesisty
- caucasion males
- smoking increases risk (not main)
Protective effects:
- fiber
- NSAIDS (seems counterintuitive)
esophageal cancer:
squamous cell carcinoma
prevalence?
location?
4 RF?
key point to remember?
prevalence is decreasing
middle esophagus
RF:
- smoking
- alchohol
- diet low in fruits and veggies
- achalasia increases risk 16 x
*** accounts for 90% of all squamous carcinoma in US***
esophageal cancers
sxs
1 early
3 late
SXS:
early:
1. transient “sticking” of food that turns to PROGRESSIVE DYSPHAGIA
later:
- retrosternal pain/burning
2.iron deficient anemia -loss from chronic cancer, but not enough to notice hememensis or occult
3. tracheobronchial fistula
late complication where the esophageal wall infilates the stem bronchus causeing intractable coughing with frequent pneumonia
_***if this occurs person has less than four weeks to live***_
in esophageal cancer, when would you expect to see the weight loss and dysphagia?
when the lumen is less than 13 mm
esophageal cancer
2 DX
2 STAGE
dx:
- barium studies
- endoscopy
Staging:
- CT OF CHEST AND UPPER ABDOMENT
2. PET SCAN
where are adenocarcinomas and squamous cell esophageal cancers found?
adenocarcinoma: lower 1/3
squamous: middle esophagus
esophageal varices

what is this?
what causes this?
mortaltiy rate?
MOST COMMON CAUSE?
emergency!!!
dilation of the submucosal veins that develop in pts with portal HTN
patho: blood flow through the liver is diminished causing blood flow increase through the microscopic bood vessesl within the esophageal wall and the vessels dilate profoundly, and then continue to dilate until they are large enough to rupture
patient acutely ill, mortality rate 40-70%
MOST COMMON CAUSE OR PORTAL HTN IS CIRROSIS that causes this

where is the most common stie for esophageal varices? why?
distal esophagus at gastroesophageal junction because veins are most superficial here!!
esophageal varices
6 sxs
3 dx
sxs:
1. hematemesis!!! over 50% stop bleeding spontaneously
- melena
- tachycardia
- hypotension
- syncope
- jaundice
DX:
1. emergent endoscopy
CBC
BUN/creatine
type and cross
esophageal varices
4 immediate tx options
- immediate tx-stop bleeding because mortaltiy approaches 75%
- visceral ligation- rubber band
- sclerotherapy
- balllon tamponade
mallory-weiss tear
what is this?
what does it occur from?
who commonly seen in?
MC location?
3 RF?
2 sxs?
linear mucosal tear in the distal esophagus or gastric cardia from forceful vomiting or retching, causing hematemesis commonly seen in alcoholics

most common location: gastroesophageal junction
RF:
alcholic
hiatial hernia
eating disorder BULEMIA
SXS:
- multiple bouts of vomiting and retching followed by PAINLESS HEMATEMESIS
- abdominal pain
***keep in mind the bleeding usually stops spointaneously as teh condition is usually benign**
mallory weiss tear
1 dx?
2 tx?
DX:
ENDOSCOPY
TX:
-
stabliazation
- transfusion/gastric lavage if needed - control bleeding via endoscopy
**keep in mind most bleeding stops spontaneously and condition is usually benign**
esophageal ring
what is this?
sxs?
dx?
1 tx?
ring of tissue located at the gastroesophageal junction called
schatzkis ring
sxs:
- dysphagia with foods, but not typically liquds
DX:
barium esophagram
TX:
mechanical dilation with balloon

in mallory weise syndrome what is somethign you want to do before releasing someone from hospital?
obtain occult negative stool to insure not bleeding still or hemmoraging
systemic scleroderma
what is this? what are the 5 common presentations? what is the #1 think you worry about in this? what test do you do in the lab? what are the treatments?
thickening and harderning of the skin via collagen deposition
- raynauds (75%)
- vascular changes in nail bed
- GI dysmotility “watermelon stomache”
- puffy hands
- fixed face
*****WORRY ABOUT PULMONARY FIBROSIS AND ACUTE RENAL FAILURE*******
DX: ANA-SPECKLED
Tx: treat system effected
renal-ACE inhibitors
raynauds-calcium channel blockers
Gi: promotility
lungs: cyclophosphamide

CREST Syndrome
what is the pneumonic to remember the symptoms and what do you need to monitor annually in these patients?
LIMITED SCLERODERMA
C- calcinosis of joints leading to puffy hands
R- raynauds
E-Esophageal dysmotility
S-sclerodactyly of MCPs
T: telangiectasis
**complication=pulmonary hypertension so need to get annual PFT/DLCO to make sure no lung fibrosis**
Tx: symptoms

stomach neoplasms
where do these occur?
appearance? 4
sxs?
3 dx?
1 tx
occur in antrum, MC in lesser curvature
bulky, irregularly shaped
firm, jagged edges
usually asymptomatic till late disease
early detection is therefore difficult
DX:
- barium swallow xray
- endoscopic studies with bx
- cytologic (screening in atrophic gastritis/polyps)
TX:
surgery-radical subtotal gastrectomy TOC
what are 6 RF for stomach neoplasms?
- genetic predisposition
- carcinogenic diet
smoked food/perserved food
- autoimmune gastritis
increased inflammation
- gastric adenomas
- polyps
- h. pylori, cofactor for some
Peptic ulcer disease

what this this?
2 causes?
1
3
size?
break in the gastric or duodenal mucosa that extends through the muscularis mucosa that comes from
1. impaired normal mucosal defense factors
NSAIDS
2. defense factors overwhelmed by aggressive luminal factors
acid
pepsin
infection
greater than 5 mm in diameter
what are the 5 common causes of PUD?
- NSAIDS
- H. pylori
- idiopathic
- hypersecretory states
- smoking
3 locations of PUD?
which one is most common?
how long do they take to heel?
what do you need to keep in mind that is very important depending on location?
- duodenal
a. MOST COMMON LOCATION!!
b. 90% heal in 4 weeks
2. pylorus
3. gastric
**CAN BE MALIGNANT**
**must get bx at endoscopy time**
a. take longer to heal 8 weeks!
b. increased length of tx
peptic ulcer disease
NSAIDS
cause?
why?
4 RF?
2 tx? length of time?
caused by long term NSAID use esp nonselective COX1 and COX2 blockers
COX1 decreases prostaglandins which have a protective effect on gastric mucosa, it the lack of this impairs gastric mucous and HCO3 secretion
**this is why COX2 selective are better option since decrease risk of bleeding**
RF:
- ASA
- corticosteroids
- over 60
TX:
1. PPI or H2
***4 weeks duodenal***
***8 weeks gastric***
2. D/C NSAID
peptic ulcer disease:
h. pylori
KEY?
characteristic?
acute/chronic characteristics?
what is key about this?!
nesscary cofactor for 75-90% of duodenal/gastric ulcers
characteristics:
PRODUCE UREASE
ACUTE:
a. infectious “gastroenteritis”
CHRONIC:
a. ASYMPTOMATIC
b. DIFFUSE SUPERFICIAL MUCOSAL INFLMMATION WITH POLYPS
**ERRADIACATION IS ESSENTIAL OTHERWISE 85% WILL RECURR!!!!!**
what is a RF for all ulcers?
smoking!
explain te patho of stomach ulcers caused by h. pylori?
- infection in body
- causes gastritis and chronic inflamation that overwhelms immune system
- causes mucosal breakdown
- creates gastric ulcer
PEPTIC ULCER DISEASE
2 sxs
3 dx
when do you use each?
1 think must do?
SXS
- epigastric like pain “hunger like” in 80-90%
- 50% have relief by eating antacids within 2-4 hours
**physical exam is often unremarkable so need to watch for changes in pattern, indicating perforation or penetration**
DX:
- endoscopy EDG TOC!
allow so for visulaization and also bx!!
- fecal antigen test (noninvasive)
- c-urear breath test (noninvasive)
****OPTIONS 2 AND THREE AT THE TOC FOR ACTIVE PUD AND PROOF OF ERADICATION*** MUST D/C PPI 7-14 DAYS PRIOR OR MAY GET FALSE POSITIVIVE!
peptic ulcer disease:
Treatment for H. pylori
what is the tx regimen?
what must you do after tx and when?
2/3 abx, PPI, +/- bismuth
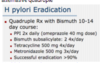
1. amoxicillin 1 g BID
2. clarithromycin 500 mg BID
3. HIGH DOSE 40 mg PPI BID
***no reason shouldn’t use quadrople therapy see in this pic** KNOW BOTH
**must confirm eradication with C-urea breath test or fecal antigen test
4 weeks post abx
2 weeks post PPI***
peptic ulcer disease
tx without h. pylori
2
3 for first
1 second
- antisecretory agents
A.PPIs 1st DOC-inhibit 90% acid secretion
ompreazole
lansoprazole
B. H2-inhibit histamine mediated secertion
C. OTC anti-secretory
- mucosal defense agents
2nd line can be used as adjunct for symptom relief
sacralfate, busmuth
peptic ulcer disease:
post H. pylori tx tx
2 considerations
DUODENAL f still large or bleeding post tx:
continue PPI for 2-4 weeks
GASTRIC if large ot blleding post tx:
continue PPI for 4-6 weeks
in reccurent ulcers what must you do!?
rule out H. pylori and NSAID use
peptic ulcer disease:
COMPLICATIONS
PENETRATION/PERFORATION
results in?
2 sxs?
tx?
results in chemical peritonitis
a. severe generalized abdominal pain
b. rigid abdominal rebound
TX:
1. laproscopic perforation closure
2. increased RX TX
peptic ulcer disease:
refractory ulcers
what is this caused by?
3 contributing factors
uncommon, contributed to non compliance with medication
Contirbutory factors:
- cigs
- NSAIDS
- failutre to eradicate H. pylori! MUST DO THIS
explain the pathophys of pacreatitis?
what are 2 theories that cause this?
- inflammation of the pancreas causes damage to the acrinar cells
- the inactive proenzymes like trysinogen are activated early while still in the pancreas
- early activated lipases disolve the fat
- so the pancreatic enzymes start to DIGEST THE PANCREASE “EATS ITSELF”
theories:
- obstruction of the pancreatic duct due to stones
- failure of the two parts of the pacreas to fully join during development pancreatic divism
acute pancreatitis
what are 2 MC causes? account for what? 6 others?
causes:
- gallstones 45%-MC
- alcohol 35%
**these two are most common and make up 80% of cases**
other causes:
trauma
drugs (iatrogenic)
obstruction (tumors)
infections (mumps)
metabolic (hyperlipidemia)
toxins (methyl alcohol, scorpion stings)
**MOST RECOVER AND HAVE NORMAL FUNCTING PANCREASE**
when dxing pancreatitis and looking at labwork, what test is most effective?
lipase
(this is better than amylase)
acute pancreatitis
5 labs tests?
TOC for dx?
LAB TESTS:
elevated cbc (infection)
elevated lipase (pancreas)
elevated LFT
elevated glucose
decreased calcium
TEST OF CHOICE FOR DX: CT SCAN!!!
scored A-E, A is good, E is bad
acute pancreatitis
6 sxs
where is pain?
severity?
what makes worse/better?
pain with…?
two key signs you dont want to miss?
- epigastric radiates to back
- billiary colic PERSISTS DOESN”T GO AWAY
- worse SUPINE, BETTER LEANING FORWARD
- PAINFUL INSPIRATION, SHALLOW BREATHS
- TACHYCARDIA
6. hemmoragic pancreatitis
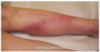
cullens sign: periumbical ecchymosis
grey tuner’s sign: flank eccymosis

acute pancreatitis
5 labs tests?
TOC for dx?
LAB TESTS:
elevated cbc (infection)
elevated lipase (pancreas)
elevated LFT
elevated glucose
decreased calcium
TEST OF CHOICE FOR DX: CT SCAN!!!
scored A-E, A is good, E is bad
chronic pancreatitis pathophysiology
what is this?
what should you think about when thinking of this?
what happens?
inflammatory disease of the pancreas
irreversible** **changes occur
can lead to permanent loss of function
HINT: think necrosis fibrosis theory of alcoholic pancreatitis
alcohol to tissue damage to fibrosis to partial obstruction
chronic pancreatitis
what is the MC cause of this?
3 others?
NOT CAUSED BY WHAT?
what can this lead to?
- alcohol cause #1!!
***THIS IS NOT CAUSED BY GALLSTONES LIKE ACUTE**
- obstructive causes of spincter of oddi by neoplasms
- malnuitirion
- metabolic
chronic pain leads to opoid addiction! keep this in mind
chronic pancreatitis
4 sxs?
sxs:
- epigastric abdominal pain that radiates to the LEFT
- insufficiency of pancreatic function leads to
a. steatorhhea damages decreases lipase
b. diabetes once islets damaged
3. asymptomatic and found incidently
chronic pancreatitis
5 tx options
most important!!
2 drugs?
- _stop the alcoho_l!!
- controls sxs
a. pain control
b. prancreatic enzyme supplements viokase and pancrease
- endoscopic duct decompression
- surgical draingage of duct
- celiac plexsus nerve block
acute pancreatitis
6 tx options?
what is the process dependent on?
mostly supportive

a. NPO 48-72 hours NO ALCOHOL
b. ERCP if presense of stone** **on CT scan
b. maintain hydration
c. pain control
d. NG tube in extreme
e. abx if infectious
f. incision and drainage if infected/necrosis
chronic pancreatitis
4 dx options
fat stranding
- amylase/lipase NORMAL

body gets used to working under these circumstances
- secretin stimulation test “gold standard” for early chronic pancreatitis dx
- plain xray films QUICK AND CHEAP-see calcifications
- CT SCAN-better at seeing calcifications but $$/rad
“arrowhead and fat stranding”
pancreatic cancer
4 sxs?
toc? 1
sxs:
- painless jaundice is PC until prove otherwise
- virchows node-supraclavicular node
- trouseaus signs- recurring superficial thrombophlebitiscan be anywhere
- weight loss
TOC: CT scan dual phase helical

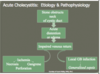
acute cholecystitis
what happens in this?
what is most likely to cause this?
leads to 3 things? possible worst case?
2 key sxs?
the cystic duct** becomes blocked **most commonly from gallstone!
less common:
cancer, sludge, infection
blockage causes distention and edema that cauess ischemia, necrosis, perforation and possible generalized sepsis
SXS
- RUQ/epigastric pain radiate to shoulder/scapula
- murphys sign (tenderness and pt stops inspiration on palpation)
acute cholycystitis
TXOC?
3 others?
TreatOT: TAKE IT OUT!! MOST COMMON!! via laproscopic cholecystectomy
- leave in if very mild
- drain it if patient too sick
- abx if elevated WBC

cholelithiasis
two types of stones?
percentage?
what do they look like?
1. cholesterol stones
MC-75% of stones!!
don’t show up on xray
- calcium bilirubinate/ca salts
25% of stones
pigmented black/brown sludge stones

acute cholithiasis
what do you need to keep in mind about sxs?
how do they present? 3
dx TOC?
what do you need to keep in mind?
asymptomatic in 50-60%

symptomatic patients:
biliary collic with RUQ pain/epigastric areas
refers to back, scapula or R shoulder
DX:
TOC: transabdominal US
shows stone without wall thickening
**keep in mind not great for stones in common bile duct**
choledolithiasis
what are the two dx/tx options?
what must you keep in mind?
- MRCP magnetic resonance cholangiopacreatogprahy ONLY DX

- ERCP-endoscopic retrograde cholangioancreatography DX AND TX so GOLD STANDARD!!
****keep in mind contraindicated in pancreatitis/cholecystomy***
celiac disease
what are 6 sxs that come with this?
explaination of the last?
- unintended weight loss

- persistently underweight
- sxs of poor nuitrition
- “failure to thrive in child”
- diarreah
-
dermatitis herpetiformis
a. intense itching
b. blisterning rashes
c. 10-15% of patients
Inflammatory bowel disease
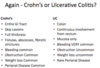
crohns disease
where are the lesions?
how deep are lesions?
where is the pain?
3 things that can occur as complications?
4 things that are common?
3 other things it can effect?
bowel appearance?
- legions mouth to anus; spread out with healthy tissue between
2. transmural
3. RLQ pain MC
- fistulas, abscesses, fibrotic stricutres
- bleeding common
- weight loss common
- obstruction common
- perianal disease common
- can effect skin eyes joints liver
- large volume diarreah and mucous (trash bag)

ulcerative colitis
where is this?
pain presents?
what is most common and worse?
what does person have increased?
what might they develop?
describe lesions and how deep?
what does the colon look like on colonscopy?
what are 3 things aren’t present?
- primarily localized in colon
2. LLQ
3. bleeding from rectum is most common
- urgency need of BM
4. potenital anemia due to blood loss
- lesions are continuous starting at the rectum and in mucosa only
- colon wall thin with continuous inflammation
- no granulomas
(weight loss/obstruction very rare with this)
colonrectal cancer
4 sxs
2 key dx
3 others
sxs:
- colic type pain
2. anorexia
3. thin appeareance
4. pallior/anemia
dx:
- xray: classic apple core/npaking ring appearance
- endoscopy with bx
- iron deficient anemia
- hypoalbuminemia
- occult blood in stool

rectal polyps
what are these?
why is it improtant to know type?
1 type concerned about?
why?
2 shapes?
small outcropping that grows in the rectum or colon
**need to deterine the type since some are associated with carcinoma**
adenomas
PREMALIGNANT POLYP
PRECURSOR TO COLORECTAL CANCER
sessile: flat and intimately attacted to mucosa
peduclated: round and attached be stalk

what is the dentate line?

senstion?
divides the rectal mucosa from the squamous epithelium in the canal
above in anorectal canal: INSENSATE (no pain)
below in andoderm: SENSATE AND PAINFUL!!
anal fissure
what is this?
where do these occur?
signicant stat?
2 causes?
Tear in the andoderm of rectal canal
90% are posterior along midline
most common cause of painful rectal bleeding
causes:
- passage or hard stool
- prolonged diarreah

internal hemmoroids

4 key sxs with these!
above the denate line!!
veins surrounded by mucosa
- PAINLESS, above denate
2. bright red bleeding with defecation
3. may prolapse and be palpable on DRE
4. bleed
what are the stages used to define internal hemmoroids?
first-bleed
second-bleed and prolapsed, spontanously reduce
third-bleed, prolapse, and require manual reduction
fourth degree-bleed/incarcerate

external hemmoroids
whe do they occur/what are they covered in?
3 sxs
dx method?
1 tx?
below the dentate line and covered with andoderm
- usually don’t bleed
- may thrombose which is VERY painful
- cause pain, discomfort and most severe at time of defecation
dx
“either present or not”
tx:
- excision of outside of the mucotaneous junction leaving wound open hemroidectomy

***what are the 2 test results you want to keep in mind when looking at hepatits infection***
hepatitis B surface antibody (HBsAB)=IMMUNITY–ONLY PRESENT IN VACCINATED PEOPLE
hepatitis B envelope antigen (HBeAg): NEEDS TREATMENT, current infection
cirrhosis
what is this?
2 classifications?
chronic end stage dxs of the liver marked by degeneration of cells from inflammation resulting in fibrous thickening of tissue
4 stages of fibrosis and cirrhosis is the last
compensated: although fibrotic can still preform functions
decompensated: fibrotic with loss of essential function