Neuro Flashcards
dementia
what are 5 key features you may find?
1, memory loss
- speech and language difficulties
- problem solving difficulties
- impaired judgement
- may have mood issues
dementia
mood issues include? 5
depression
agitation
delusions
insomnia
disinhibition
what are 3 neurological features that might help explain the neuro changes seen in dementia?
- changes in cerebral circuits
- nerve loss
- changes in neurotrasmitters
what is the most common form of dementia?!
alzheimers
what are the 8 causes of the different types of dementia?
- alzheimers
- vascular dementia
- multi-infarct dementia
- frontotemporal dementias (huntingtons)
5 parkinsons dementia
- dementia with lewy bodies
- ETOH/drugs
- viral (creutzfeld-jakob)
what are the two most common forms of dementia?
1- parkinsons dementia-50%
alzheimers dementia
what to keep in mind about htis?
what causes this? 2
do they know they have it?
most common dementia
memmory loss can start as very subtle
progressive over years
NEURITIC PLAQUES (senile plaques)** and **amyloid deposition in arterial walls of neurons making neurofibillary tangles “neurons get all tangled up so they don’t work as well”
don’t recognize that they have it
behavior changes, may get lost
who is there a higher incidence of alzheimers dementia in?
down syndrome pts
alzheimers dementia
8 presentations
- word finding issues/speech difficulties
- wandering/getting lost
- poor judgement
- delusions
- agression
- sleep disturbance
- incontinence
- bedriddent status
alzheimers disease
why is it difficult to dx?
you can only confirm on autopsy with brain bx
what are the 3 most important risk factors for alzheimers dementia?
- OLD AGE—–most important RF
- family hx
- female gender
how do you confirm alzheimer on autopsy?
apolipoprotein 4 on autopsy
vascular dementias

what to remember about this?
who do you find this in?
what are the type?
SECOND MOST COMMON DEMENTIA
multi-infarct dementia in classically HTN pts
small or large infarcts known as lucunar** **and multiple cortical infarctions
**more sudden onset**
frontotemporal dementia
what is this caused by?
4 early sxs? what comes later?
what are 3 diseases that cause this?
caused by degeneration of the frontal (behavior) and temporal lobe
early features include:
- attention issues
- judgement impairment
- awareness
- behavior issues
***memory loss seen in later disease***
- huntingtons chorea
- picks disease
- progressive supranuclear palsy
huntington’s chorea
inheritance pattern?
where is defecT?
autosomal dominant-50% chance for kids
chromosome 4
frontotemporal dementia:
picks disease
what does this result in?
what do you see on testing?
tx?
anterior frontal and temporal cerebral cortex with MARKED personality changes
***intracellular inclusion (pick bodies) stain with silver stain
Tx:
NONE
tx behavior
what are the lewy bodies that are seen in dementia?

intaneuronal cytoplasmic includsions that stain with PAS staining
demenia:
progressive supranuclear palsy
what are 4 things this is qualifed by?
how long does the person have to live?
tx?
- falls
- gaze paralysis cant look down
- rigidity
- dementia
death within 5-10 years, no tx
dementia:
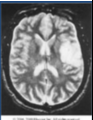
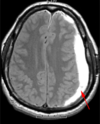
normal pressure hydrocephalus
what are 3 sxs?
2 dx methods?
1 tx?
- gate ataxia
- dementia
- urinary incontinence
**think falling adult who is incontinent**
DX:
- LARGE VENTIRICLES ON IMAGING/CT
- sume use MRI or CSF tap
tx: shunting
dementia:
korsakoff syndrome
what is this?
can’t recall recent memory despite immediate memory retention
easily confusable
what is a vitamin deficiency that can cause dementia?
B12…macrocytic anemia…causes spinal cord issues “myelepathy”
REPLACE IT
dementia
5 workup you want to do
- history
- mini mental exam
- full neuropsychiatric testing
- B12, thyroid function
- consider CT/MRI to turn our tumor/infarction
dementia
3 tx options for the actual dementia itself
- anti-acetylcholinesterase
**increase ach by inhibiting cholinesterase**
effects last about a year
- donepexil (aricept)
- galantamine
- riovastgmine
- NMDA receptor antagonists
**blocks this over-excitatory neurotransmitter**
used for mod to severe disease WITH ANTI-CHOLINESTERASE DRUGS
- Memantine (namenda)
- COMBO MEMANTINE PLUS DONEPEZIL for alzheimer dementia “Namzaric”
***all can be used in AD or parkinson’s dementia***
what are the goals of txing dementia with medication?
- delay progression of the disease
- improve caregiver disease
- decrease agitation
**can be used in AD and parkinsons…outcomes not as good in other dementia forms**
dementia
tx options for behavior
VERY DIFFICULT
antipsychotics:
- haloperidol
- resperidone
delirium
what is this?
how long can it last?
what are 3 things it can be attributed to?
acute confusional state with decreased attention
hours to days, even months-years
1. usually due to cerebral dysfunction
2. can be abnormal acetylcholine levels
3. high dopamine
**can minic dementia**
what are 4 things that can cause delirium?
- older age
- baseline dysfunction
failing health, dementia, nursing home pts
- poor sleep
- hospitalizations
catheters, restraints, sleep deprevation, multiple meds, pain
delerium:
ICU psychosis
what is this?
4 causes?
r/o?
illness
(sepsis, fever, dehydration, drug abuse)
must rule out stroke
delerium:
sundowning
what is this?
2 tx options?
old people get worse at night
tx:
- maintain day-awake, night sleep
- reassurance/reorientation
delerium:
alcohol withdrawal/delirium tremens
what are these and when are they the worst?
4 sxs?
5 tx options?
delirium temors stem from acute alcohol withdrawal and peak 2-3 days after cessation
SXS:
- agitation/axiety
- tremor
- hallucinations
- ANS instability (increased BP, pulse, resp)
TX:
- B vitamins
2. hydration
3. benzodiazepines
a. diazepam
b. chlordiazepoxide
IV or PO
c. high dose benzos for bad DTs
4. phenobarbitol
5. antipsychotics
a.haloperidol
delerium:
5 presentations and whicho ne is most important?
- decreased attention
- change in sleep/wake cycles
- hallucinations
- delusions
- hypo/hyperactive status
delerium
what are 3 dx options?
what are 5 tx options?
dx:
- clinical at bedside
- compare baseline function (ask family)
- check for meidcations causes (anticholinergics, sedatives, narcotics, benzos)
Tx:
- supportive/reorientation
- day-night normalcy
- bed alarms, sitters
- antipsychotics- haloperidol
- benzodiazepine-diazepam
VERY DIFFICULT
seizure
what are the two maine categories of this?
what causes each?
1
3
partial:
a. deranged area of the cerebral cortex often due to STRUCTURAL ABRNOMALITY CONCIOUSNESS IS PRESERVED
**keep in mind in the subcategory of this complex partial conciousnesses is IMPARIED=PARADOX..it just doesn’t make sense**
generalized:
a. diffuse region of the brain firing
b. often widespread problem:
- cellular disorder aka mental retardation
- biochemical disruption: low Na
- structual: brain tumor
PARTIAL:
SIMPLE PARTIAL SEIZURE
9 sxs of this
2 dx
sxs:
- no loss of conciousness
- isolated** **tonic/clonic with repetitive flexion and extension
- hand tremor on opposit side of issue
- jacksonian march
motor activity begins distally like fingers and spread through entire extremity, can lead to entire side of body
- todds paralysis
local parethesia lasting minutes to hours
6.changes in somatic sensations (parersthesias)
7. changes in vision (flashing lights, hallucinations)
8. changes in equilibrium (falling, vertigo)
9. autonomic changes (flushing/sweating)
DX:
EEG spike waves in FOCAL area of the brain or during jacksonian march
PARTIAL:
COMPLEX PARTIAL SEIZURE
what are 3 sxs with this? 3 examples
SXS:
- impaired conciousness, loss of contact with environment “ictal stage”
a. STARING-kinda asleep and staring off into space, can’t wake them
b. AMNESIA-forgetting/impaired memory
c. involuntary picking/chewing
- preceeding aura
- post ictal confusion
Lasts seconds to hurs, EEG notmal between spells
PARTIAL:
partial with secondary generalization
when does this occur?
what type of seizure does this produce?
electrical discharge spread and both hemispheres become involved
TONIC CLONIC SEIZURE
common when partial seizures occur in the frontal lobe
GENERALIZED:
absence seizures-petit mal
who does this occur in?
when do they stop?
3 sxs with 5 subtle findings?
1 DX with 3 findings?
childhood 4-8 years, 15-20% of childhood seizures, MOST RESOLVE IN CHILDHOOD
NO CONVULSIONS
- LOSS OF CONCIOUSNESS
- few seconds
- subtle findings
eye blinking
FACIAL TWITCHING
chewing
clonic movement of hands
all day long daydreaming appearance
DX:
- EEG
- general symmetrical discharge
- spike and wave
- WORSEN WITH HYPERVENTILATION MANEUVER
GENERALIZED:
atypical absence seizures
what differentiates these from absence seixures?
who might they occur in? 2
same as absence but LAST LONGER with more motor features
may have brain abnormlaity like mental retardation or developmental delay
HARDER TO TX
GENERALIZED: generalized tonic/clonic seziures “Grand mal”
What is this most commone cause of this?
How fast do they occur?
6 sxs seen?
10% will have epilepsy
caused by metabolic derrangement
SUDDEN ONSET
SXS:
- convulsive
- increased muscle tone stiff
- moan or cry
- change in respiration (secretions, cyanosis, jaw clench)
- clonic activity: muscle relax and contract
- post ictal state:
unresponsive,
flaccid,
salivation/airway obstruction, bowel/bladder incontinence
GENERALIZED:
tonic-clonic Grand mal seizures
what do you find on the EEG between the two phases?
dX EEG:
tonic phase:
increased low voltage fast activity
high amplitude polyspike discharge
clonic phase:
spike and wave activity develops
GENERALIZED:
tonic-clonic Grand mal seizures variation
myoclonic seizure
what is this?
who do you see this in?
brief contraction or jerk like when you fall asleep and twitch
*seen in brain injuries*
Generalized:
juvenille myoclonic seizure
who is this in? does it go away?
1 sxs?
when is it worse? 2
adolescence, spontaneous remission
billateral jerk with maintained conciousness
worse with awakening and sleep deprevation
GENERALIZED:
lennox gastaut syndrome
who is this in?
what are 4 things it is associated with?
children!!
impaired cognitive function
associated with CNS:
developmental delay
trauma
infection
neural injuries
GENERALIZED:
mesial temporal lobe epilepsy
what is the dx for this?
MRI shows hippocampal sclerosis
explain the patho of seizures?
6 steps
- burst of electrical activity
- influx of calcium, aided by NMDA
- influx of sodium, aided by GABA or K channels
- spikes discharge
- inhibitory neurons overloaded with calcium and k
- propogation of action potentials
what can seizures come from?
1 theory?
5 causes?
harrisons: shift in balance of excitation and inhibition of the CNS
- change in seizure threshold
- genetic role
- traumatic brain injury
- strokes infection
- stress, sleep deprevation, menses, medications
febrile seizures
who does this occur in?
3 associations?
how many?
3 months-5 years
infection related:
ottitis media
respiratory
gastro
can be complex (multiple) or simple (single)
what causes 50% of new seizures in adults?
cerebrovascular disease
how do you dx a seixure?
4 (+findings)
- hx is key, from bystander or witness
- EEG: starts or stops abruptly activity during tonic-clonic inter-ictal-spikes or sharp waves
- sometimes MRI
- blood test, elevated prolactin in the first 30 mins
seizure tx
3 tx options?
specific medicaitons? 6
- MEDICATION MANAGEMENT
- CARBAMAZEPINE
-PHENYTOIN
-lamotrigine
-valproic acid
-gabapentin (partial)
-pregabalin (partial)
- SURGICAL
- temporal lobectomy
- focal lesion removal - VAGAL NERVE STIMULATOR
- put electrode in vagus nerve, increases the seizure threshold

status epilepticus
what is this and how long does it last?
is this serious? why? 3
5 causes of this?
continuous seiziure
15-30 mins
MEDICAL EMERGENCY
- cardiovascualr implicaitons
- hyperthermia
- CNS injury
causes:
metabolic problems
drugs
CNS infection
head injury
refractory epilepsy
status epilepticus
4 tx options?
dx: metabolic workup
Tx:
- benzodiazepine ( lorazepam, diazepam, midazolam)
2. phenytoin
3. phenobarbital
4. anesthesia
multiple sclerosis
what is this caused by?
when does it start?
who is it more common in?
what are the 5 types?
autoimmune that causes inflammation and demyleination of the CMS which makes the neurons not able to function
onset usually 20s to 30s
more common in women, more severe in men
types:
- CIS
- RRMS
- Primary progressive
- secondary progressives (SPMS)
- progressive relapsing
what are 5 RF for multiple sclerosis?
- northern europe
- southern canada
- northern US
- western europe in temporate zones
- family hx

multiple sclerosis:
relapsing remitting MS
ehsy is the pattern of this?
5 things it can lead to over time?
6 sxs?
an initial episode then months or years later sxs emerge or previous sxs return for more than 24 hours
cycle of incomplete reission and progressive disability
- weakness
- spasticity
- ataxia in limbs
- impaired vision
- urinary incontinence
despite remission steady decline still dominates the disease course
sxs:
optic atrophy
nystagmus
dysarthria
cerebellar deficits
uhthoffs pnehomenon-SXS GET WORSE IN HOT ENVIRONMENT!!!
internuclear opthalmaplegia-eye move independent
think sensory issues in teh limb followed by vision change

multiple sclerosis:
secondary progressive (SPMS)
what is this?
most patients will progress to this
initial relapsing-remitting that sudddenly begins to have decliend without periods of remisssion (gets more disabiltiy)

multiple sclerosis:
progressive relapsing
what is the pattern of this?
steady decline since onset with superimposed attacks

multiple sclerosis:
10 sxs of this
- numbess/weakness
- numbness and tingling
- unsteadiness in th limb
- spastic paralysis
- retro neuritis/ optic neuririrs
-sudden color loss
-impaired night vision
-pain with eye movemtn
-blurred or dimmed vition
6. vertigo
7.urinar incontinence from loss of spincter control
8. interneuclear opthalmaplegia (eyes move independently)
9. uhthoff pnenomenon-gets worse in the heat
10. l’hermettes syndrome: shock like feeling throughout body

multiple sclerosis:

3 dx methods/criteria?
what do you find on each?
- mcdonald criteria:

2 or more different** areas in central white matter in the brain that are **affected at differnt times
***aka you get two lesions on imaging at different times**
- MRI IS TOC FOR THIS!!:
SEE PLAQUE THAT IS REGION OF DEMYLEINATION WITH PRESEVED AXON
**FIND LESIONS IN: PERIVENTRICULAR, JUXTACORTICAL, INFRATENTORIAL, OR SPINAL CORD**
- LUMBAR PUNCTURE
a. oligoclonal bands highly suggestive of MS
b. lymphocytosis
c. albumin (disruption of BBB)
multiple sclerosis:

what is the goal of txing?
for acute attacks?
what are the three choices?
goal: improve quality of life and limiting disabiltiy!! NOT ACTUALY TREATMENT FOR CURE
acute attacks: glucocorticoids aka methylprednisone
initials DOC options for RRMS:
1. injection with interferon or glatiramer “SAFTEY OPTION”
2. oral therapy with dimethyl fumarate or teriflunomide “CONVIENCE OPTION”
3. infusion therapy with natalizumab “EFFICACY OPTION”
****keep in mind there is no right way to do this!!!….its a crap shooot because there aren’t guidelines!!***

potenital for a Multiple sclerosis cure

what is the option?
what is included in this? 2
what is the benefit of htis?
stem cell treatment (HALT-MS)
high dose immmunosuppresive tx WITH stem cell transplant
by rebooting the immune system it doesn’t seem to attack itself anymore
- 86% without relapses
- 91% without progression
ischemic stroke:
origin:
athrosclerosis
what vessels are involved?
accounts for what percent of ischemic strokes?
4 MC origins?
outcome dependent on what 3 things?
Large vessels often involved
50% of ischemic strokes
thrombus in situ (stays in the artery that it is formed and happens frequent in carotids) vs artery to artery embolus (breaks off carotid and goes into brain)
most common locations:
aorta
carotid bifurcation
origina of internal carotid
external carotid
**outcome dependent on: adequacy of collateral circulation, circle of willis, and duration of ischemia**

ischemic stroke:
Cerebral/cardioemboli
where do these come from?
make up what percent of ischemic strokes?
what two arteries does it commonly effect?
2 conditions that increase risk?

embolism from carotid to brain or heart to brain and occludes distal artery in brain
20% of ischemic strokes originate form the heart
***often effect the MIDDLE CEREBRAL ARTERY (MCA) OR ANTERIOR CEREBRAL ARTERY (ACA)
afib or atrificail valve common causes (hence why they are heavily anticoagulated)

ischemic stroke in middle cerebral artery (MCA)

what are the 4 ares you should think of when you think of being effected?
what are 5 sxs of blockage of proximal MCA?
what are the two sxs present wtih each subdivision blockage?
damage depends on what part of the MCA is affected, can be proximal or one of the two divisions
effects of GENERAL MCA BLOCKAGES:
THINK HANDS/FACE/TRUNK/SPEECH CENTER
- contralateral hemiplegia** (loss of movement) and **contralateral (loss of feeling)
- inital 1-2 days gase preference towards infarcted side of brain
- hemianopia: visiual field defect
- if stroke occurs in dominant hemisphere (aka they are right handed and occurs in left hemisphere) can lead to aphasia like above
- if stroke occurs in nondominant hemisphere: (aka they are right handed and occurs in right side of brain) anosognosia** where speech and language are preserved but get **neglect and denial of deficit or confused state** (aka don’t know something is wrong with their arm etc) can cause **construction apraxia where they can’t draw or construct 2 and 3D images
EFFECTS IF DIVISION OF MCA IS EFFECTED/BLOCKED
SUPERIOR DIVISION:
1. contralateral motor and sensory loss
2. BROCAs aphasia: non-fluent (expressive) aphasia, can understand language but can’t speak fluently or create sentences
iNFERIOR DIVISION:
- WERNICKES (fluent) aphasia: inability to comprehend spoken language the CAN speak but what they have a hard time getting what they want to say out, speech may lack meaning
2. homonymous hemianopsia: loss of half the field of view on the same side in both eyes
ichemic stroke in anterior cerebal artery (ACA)

what areas are the most common effected? 2
7 sxs of this including 2 reflexes?
THINK FEET/LEGS
less common than MCA
***if occluded proximal to anterior communicating artery, very little sxs because the cicle of willis takes over if intact***
- paralysis of contralateral leg
- urinary incontinence
- GRASP REFLEX: stroke skin between thumb and index finger, if positivie cuases the patient to grasph finger
- SUCK REFLEX: stroke center of the lips/tongue, if positive causes sucking movement by patient
- abulia: slowness to respond; lack of spontaneous movement
- impariemnt of grait!!
7. behavior changes/memory distrubance
ischemic posterior circulating stroke

what arteries can this effect? 2
3 general sxs?
4 sxs of total occlusion?
7 sxs of a partial occlusion?
least common, often asymtomatic if cirlce of willis in intact
vertebral artery (branch of subclavian) or basilar artery
sxs
- homonymous hemianopsia
- contralateral motor/sensory loss
- ipsilateral bulbar/cerebellar signs
TOTAL OCCLUSION (very serious)
- pinpoint pupils
- flaccid quadriplegia
- sensory loss
- loss of cranial nerves
PARTIAL OCCLUSION
- vertigo
- ataxia
- dysarthia (loss of control of tongue)
- diplopia
- visual loss
- weakness of sensory loss in the extrememites
- CN disturbances
what to do you do dx stroke?

- CT to r/o hemmorage
don’t usually see the infarcts on CT, only 5% visible in first 24 hours which is why you have to go to the next stage!!
- Angiography “gold standard” and most acurate
- MRA-noninvasive
replaces need for angiogram in some patients
hemmorhagic stroke:

INTRACEBRAL HEMMORAGE
what are the vessels that are involved?
4 things it can quickly lead to?
mortality rate?
RUPTURE OF SMALLE ARTERIES OR MICROANEURYSM OF THE PERFORATING VESSELS
RAPID PROGRESSION OF NEUROLOGIC DEFICIT
OFTEN PROGRESSING TO
HEMIPARESIS
HEMIPALEGIA
HEMISENSORY LOSS
LOSS OR IMPAITED CONCIOUSNESS 50%
50% MORTALITY
hemmoragic stroke:
subarachnoid space
what are the 2 causes? MC?
5 key sxs to look for?

CAUSES:
MC BLEEDING FROM SACCULAR ANEURYSMS “BERRY ANEURYSM” 75% of cases
AVM
sxs:
- MOST SEVER HEADACHE-THUNDERCLAP
- followed with N/V
- nuchal rigidity
- positive kernigs-can’t extend leg when lifted
- positive brudzinskis sign-lift head causes knees to rise
***kernigs and brudzinskis are positive in meningitis but are also positive here!!**
- fever up to 102

what are the 2 dx for hemmorhagic stroke? finding?
- CT showing hemmorage
if neg
- spinal tap to r/o subarachnoid hemmorage via presence of blood or xanthochromia

epidural hematoma (hemmorage)
where does it occur?
MC cause?
presentation on CT? 2
between skull and dura

MC-skull fracture
CT: convex lense shaped lesion usually in temporal area and doesn’t cross suture line
subdural hematoma (hemmorage)
what type of blood and from what vessel?
MC MOA?
image on CT? 2
venous bleed between dura and arachnoid MC from tearing of bridging veins
MC blunt trauma, contre coup and causes bleeding on opposit side of injury
CT: concave cresent shaped and can cross suture lines
parkinsons disease
what is the patho of this?
4 cardial signs?
3
3
4
3
neurodegenerative disorder resulting from diecrease dopaminergic transmission in basal ganglia parkinsons think dopamine
four cardinal sxs:
1. TREMOR
occurs in 85%
resting tremor, PILL ROLLING
one limb or one side for months to years
spares head
2. RIGIDITY
iincreased reistance to passive movement COGWHEELING rigidity
no weakness!!!!!!!!!!!!
no change in DTRS!!!!!!!!!!!!!!!!!
3. BRADYKINESIA
slowness to get moving “start hesitation”
effects voluntary movements and speech
4. POSTURAL IMPAIRMENT
difficulty with balance and gate
stooped over, leaning forward
occurs later in disease course
fenesterating gate, with stopping on turns
fast short steps

Cerebral Palsy

what is this?
3 options of presentation?
SXS
2
1
4
involuntary sustained or intermittent muscle contractions cause twisting and repetitive movements, abnormal posture or both
presentaiton:
- arm and leg on one side (hemiplegic)
FLOPPY OR SPASTIC HAND
WALKS ON TIP TOE OF EFFECTED SIDE
- both legs only (diplegic)
CONTRACTURES OF THE ANKLES AND FEET
-
both arms and both legs (quadriplegic)
- ARMS HEAD AND MOUTH MAY TWIST STRANGELY
- SEVERE BRAIN DAMAGE THEY CAN’T WALK
- KNEES PRESS TOGETHER
- LEG AND FEET TURN INWARD

myasthenia gravis PE
two signs you can see while doing tests in the exam room? 2
- _simpson test-_drooping eyelid with forced upward focus from fatigue

- cogan lid twitch: follow finger and they get fatigue of the eyelid and it drops
myasthenia gravis

what are the 5 tests you want to do?
which 2 would be the 2 tests you would want to make sure to do?
1. Tensilon test
give short acting AchR inhibitor–allows for the ACH to stay around more and it fixes the fatigue (pick on the front)
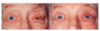
2. Ice pack test
neuromuscular transmission improves at cold temps and the muscle fatigue disipates (pic on this side), 80% sensitive
3. antibody against NAchR (nicotinic ACH receptors)** **THIS IS THE FIRST THINK YOU WOULD REALISTICALLY DO!!
80-90% have this
4. CT/MRI of the thymus DO THIS FOR EACH PATIENT AS WELL
5. repetitive nerve stimualation studies
duchenne muscular dystrophy
what is this?
who does it occur in?
onset? progression? Life expectancy?
3 sxs? progression?
1 tx?
defective X chromosome so THEY DON’T PRODUCED DYSTROPHIN (leading to enzymatic breakdown of the muscle)
occurs in males, females asymptomatic carriers
ONSET: 2-3 years old
may be wheelchair bound by 12
life expectancy into 20s
SXS:
start on trunk and spread to extremities
- cardiomyopathy
- scoliosos
- fractures from falls
DX:
ELEVATED CK
TX: CORTICOSTEROIDS

beck muscular dystrophy
wha tis this and how is it different than DMD?
genetic link?
survival age?
spread of sxs?
1 tx?
similar to DMD, but
they make some dystrophin
-defective X chromosome
age of onset leter than DMD
likely elevation of CK
survival into 40s
sxs:
start on trunk and spread to legs
-can effect the heart
TX: corticosteroids

emery-dreifuss muscular dystrophy
who do you find this is?
exaplin the sxs spreading pattern?
classic triad….what is this?
3 dx options?
unique to know about this?
many different inhertance patterns and in BOTH men and women
SXS:
MUSCLE WEAKNESS BEGINS IN ARMS AS TEEN AND PROGRESSES TO LEGS AND FACE
TRIAD:
1. CONTRACTION OF THE ELBOWS, PLANTOR FLEXORS, AND SPINE
2. HUMEROPERONEAL WEAKNESS
3. CARDIAC ABNORMALITIES (ARRYTHMIA, CARDIOMYOPATHIES)
DX:
- CK slightly elevated
- EMG
- genetic testing
*****STILL AMBUATORY 20 YEARS AFTER SX****

myotonic dystrophy
what is this?
in who?
3 sxs? (where)
3 dx techniques?
most common form of MD

males and females
SXS:
- muscle siffness
- inability of muscles to relax after contraction **shaking somones hand and can’t get go**
- muscle loss and weakness
- facial
- arms/legs
- cardiac complications
- caracts
- abnormal intellectual functioning
DX:
- slightly elevated CK
- genetic testing
- clinical findings
facioscapulohueral muscular dystrophy
who is this in?
genetic pattern?
2 main findings?
1 main dx 2 others?
males and females
autosomal dominant
profound facial weakness “pouting appearance”
progresses to include shoulders/hips (WC bound by 9-10)
DX:
- as patient try to push up and sip up
- slightly elevated CK
- genetic testing
