3 - GI Presentations Flashcards
What organs cause acute abdominal pain in each of the four quadrants, the epigastrium and the suprapubic area?
Also consider lungs, cardiac, testicular and gynaecological pathologies, DKA

What is an acute abdomen and how do you assess a patient with this?
Sudden onset of severe abdominal pain
Need to decide if patient is critically unwell and needs surgical intervention so check observations and observe patient from bed with ABCDE
What are some causes of acute abdomen that require immediate urgent intervention?
- Intraabdominal bleeding
- Perforated viscus
- Ischaemic bowel

Intraabdominal bleeding is a pathology that presents as acute abdomen and requires urgent intervention as it can cause hypovolemic shock. What are some causes of this type of bleeding and how will a patient present with this?
- Ruptured AAA
- Ruptured ectopic pregnancy
- Bleeding gastric ulcer
- Trauma.
- Hypovolemic shock: tachycardia, hypotensive, cold to touch, clammy and pale

A perforated viscus is a pathology that presents as acute abdomen and requires urgent intervention as it causes peritonitis. What are some causes of this and how will a patient present with this?
- Peptic ulceration
- Small or large bowel obstruction
- Diverticular disease
- IBD
Patients will lay completely still with generalised peritonitis (unlike renal colic where they will be moving to get comfortable)

Ischameic bowel (Acute Mesenteric Ischaemia) is a cause of acute abdomen that requires urgent surgical intervention. How will this present in a patient and how is it diagnosed?
Severe pain out of proportion to clinical signs has ichaemic bowel until proven otherwise
Exam often remarkable but diffuse constant pain. Often acidaemic, have a raised lactate and are physiologically compromised
Definitive diagnoses via CT with IV contrast

How does colic present?
Pain that crescendos to become very severe and then goes away completely
e.g biliary colic, ureteric colic, and bowel obstruction.
What is peritonism?
Localised inflammation of the peritoneum, usually due to inflammation of a viscus that then irritates the visceral then parietal peritoneum
Pain starts in one place (visceral) then moves to another place/becomes generalised (parietal)
e.g appendicitis
What labatory tests and imaging should you do for all cases of acute abdomen?
Lab Tests
- Urine dipstick ±MC&S: check for signs of infection, haematuria, pregnancy
- ABG: for bleeding or septic patients. Look at O2, rapid Hb, lactate to see perfusion of organs
- Routine bloods: FBC, U&Es, LFTs, CRP, amylase and a group and save if likely to need surgery soon
Imaging
- eCXR: for pneumoperitoneum or lower lobe lung pathology
- US: see image
- CT
- ECG: to rule out cardiac pathology causing referred pain

What may a raised serum amylase level mean in a patient with acute abdomen?
- 3x normal limit: pancreatitis
- Raised but not 3x: perforated bowel, ectopic pregnancy, or diabetic ketoacidosis (DKA)
How is acute abdomen managed generally before a diagnosis is made?
- IV access +/- fluids
- Nil by mouth
- Analgesics
- Antiemetics
- Initial imaging, bloods and urine dip
- VTE prophylaxis
- Consider NG tube and catheter if unwell to monitor fluid balance

What are the key principles of making surgical incisions?
- Incisions should follow Langer’s lines where possible, for maximal wound strength with minimal scarring
- Muscles should be split and not cut (where possible)

What are the incisions used for an appendectomy?
Made at McBurney’s point (2/3 from umbilicus to ASIS). Passes through passing through all of the abdominal muscles, transversalis fascia, and then the peritoneum to the abdominal cavity
Lanz Incision: transverse incision that follows Langer lines so more aesthetically pleasing and less scarring
Gridiron incision: oblique (superolateral to inferomedial)

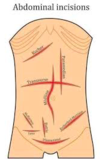
What are the names of the following incisions?

- Midline
- Paramedian
- Kocher
- Chevron / rooftop incision or modification
- Mercedes Benz incision or modification
What is a midline incision used for?
Anywhere from the xiphoid process to the pubic symphysis, passing around the umbilicus
Will cut through skin, subcutaneous tissue, fascia, linea alba and tranversalis fascia, peritoneum before reaching the abdominal cavity
Can be used for emergency procedures as good visualisation. Also minimal blood loss and nerve damage. However bad scarring

What is a paramedian incision?
Rarely used but when used it is to get to lateral viscera like kidneys and spleen
2-5cm lateral to the midline, anterior rectus sheath is separated and moved laterally, before the excision is continued through the posterior rectus sheath (if above the arcuate line) and the transversalis fascia, reaching the peritoneum and abdominal cavity
Takes a long time but prevents division of rectus muscle. However can damage lateral muscle blood and nerve supply causing atrophy of muscle medially

What is a Kocher incision and what is it used to gain access to?
Subcostal incision used to gain access to gall bladder for the biliary tree.
Runs parallel to the costal margin, starting below the xiphoid and extending laterally.
Pass through all the rectus sheath and rectus muscles, internal oblique and transversus abdominus, before passing through the transversalis fascia and then peritoneum to enter the abdominal cavity.
Heals well
What are two modifications of the Kocher incision and what are they used for?
Chevron / rooftop incision
- Extension of Kosher to the other side
- May be used for oesophagectomy, gastrectomy, bilateral adrenalectomy, hepatic resections, or liver transplantation
Mercedes Benz incision
- Liver transplantation

What laparoscopic port site is almost always the same in every surgery?
Umbilicus for camera port
Common instruments include camera, cutting and dissecting scissors, and grippers
What are some of the causes of haematemesis?
Emergency (due to haemorraghe)
- Oesophageal varices: often due to portal hypertension from alcohol abuse. Needs urgent OGD
- Gastric ulceration: erosion into blood vessels, usually lesser curve of stomach and posterior duodenum. May have history of epigastric pain, NSAIDs, H.Pylori
Non-emergency
- Mallory-Weiss Tear: just needs reassurance and monitoring. If severe or prolonged this warrants OGD
- Oesophagitis: due to GORD, infections such as candidiasis, radiotherapy, Crohn’s, ingestion of toxic substances
- Gastritis, Gastric malignancy, Meckel’s diverticulum

When a patient presents with haematemesis, what do you need to find out in the history?

See image but also check for peritonism, epigastric tenderness, evidence of underlying cause e.g liver stigmata

What investigations are done when a patient has haematemesis?
- Routine bloods (FBC, U&Es, LFTs, and clotting) and VBG
- Group and Save and crossmatch 4 units of blood
- OGD is definitive, within 12 hours
- Erect CXR if suspect perforated peptic ulcer
- CT abdomen with IV contrast if too unwell for OGD or if OGD is unremarkable

What is the Glasgow-Blatchford Bleeding Score?
Decide whether Upper GI bleed can be managed as outpatient or inpatient with endoscopy
Rockall Score (severity score for GI bleeding post-endoscopy)
What is the best imaging for acute abdomen and haematemesis?
Acute Abdomen: CT with IV contrast
Haematemesis: OGD
How is haematemesis due to peptic ulcer disease and oesophageal varices managed?
- Initial: 2 large bore IV cannulas, start fluid resuscitation if needed, and crossmatch blood
Endoscopy:
- Peptic ulcer disease: Injection of adrenaline and cauterisation or embolisation of gastroduodenal artery. High dose IV PPI +/- eradication therapy
- Oesophageal varices: prophylactic antibiotics and Terlipressin.
Endoscopic banding, Somatostatin analogues (e.g. octreotide) or vasopressors (e.g. terlipressin), Long-term repeated banding and long term beta blockers
What is the aetiology of dysphagia and what are some questions you should ask someone with this?
- Is there difficulty in initiating the swallowing action?
- Do you cough after swallowing?
- Do you have to swallow a few times to get the food to pass your throat?
Ask about regurgitation, the sensation of food becoming ‘stuck’, hoarse voice, weight loss, referred ear or neck pain

How is a dysphagia presentation investigated?
- URGENT OGD and biopsy to rule out malignancy
- FBC
If endoscopy normal can arrange manometry and 24hr pH studies to look for motilitity disorders, or barium swallow to look for pharyngeal pouch

How is dysphagia managed?
- Treat underlying cause e.g excision/palliation for malignancy
- Involve speech therapists and dieticians early if ongoing
What is a closed loop obstruction?

Why is urgent fluid resuscitation required in a bowel obstruction?
Once the bowel segment has become occluded, dilatation of the proximal limb of bowel occurs, resulting in an increased peristalsis of the bowel.
This leads to secretion of large volumes of electrolyte-rich fluid into the bowel (often termed ‘third spacing’).
What is the aetiology of small and large bowel obstructions?
Small bowel – adhesions and hernia
Large bowel – malignancy, diverticular disease, and volvulus
SURGICAL SIEVE: outside, within the wall, within the lumen

What are some clinical features of a bowel obstruction?
- See image for features
- Examination: abdominal distension, focal tenderness, tinkling bowel sounds on auscultation, tympanic sound on percussion
- Patients develop guarding and rebound tenderness with abdominal tenderness when ischaemia of the bowel is starting

What are some differential diagnoses for bowel obstruction?
- Pseudo-obstruction
- Paralytic ileus
- Toxic megacolon
- Constipation
What investigations are done if you suspect a bowel obstruction?
- Urgent bloods and a G+S due to third spacing
- VBG to look for raised lactate (ischaemia) or metabolic derangement due to vomiting/dehydration
- CT with IV contrast is imaging of choice
- AXR
- Water soluble contrast study (gastrograffin) in small bowel obstruction from adhesions from surgery

Why is CT imaging better than AXR for bowel obstructions?
(1) more sensitive
(2) can differentiate between mechanical obstruction and pseudo-obstruction
(3) can find site and cause of obstruction so good for operative planning
(4) presence of metastases if caused by a malignancy
What would you see on an AXR of a bowel obstruction?


How is a bowel obstruction managed conservatively?
- If closed loop or signs of ischaemia need urgent surgery
- If no signs of ischaemia DRIP AND SUCK (see image)
- Water soluble contrast study if does not resolve within 24 hours conservative management.

What is the surgical management of a bowel obstruction?
- Indications of surgery (see image) plus virgin abdomen
- Laparotomy
- Resection of bowel if ischaemic and anastomose or stoma

What are some complications of bowel obstruction?
- Bowel ischaemia
- Bowel perforation leading to faecal peritonitis (high mortality)
- Dehydration and renal impairment
What is a red flag that ischaemia may be developing in a suspected bowel obstruction?
- Colicky pain that becomes constant in nature or worse on movement
- Guarding and rebound tenderness
What is the aetiology of GI perforations?
- Most common: peptic ulcers and sigmoid diverticulum
- Others: sigmoid volvulus, colorectal cancer, appendicits, colonoscopy, UC in toxic megacolon
- Inflammatory, Ischaemic, Trauma

What are some of the features of a GI perforation?
- Rapid onset sharp pain
- Systemically unwell with septic features
- May have signs of peritonism, if generalised needs surgery (rigid abdomen)
- If thoracic perforation (e.g oesophageal rupture) may have chest or neck pain radiating to back, worsening on inspiration. May be vomiting and respiratory symptoms (signs of pleural effusion or palpable crepitus)

What are some investigations you should do if you suspect a GI perforation?
- Baseline bloods with G+S: raised CRP and WCC`
- Urinalysis: to rule out renal and tubo-ovarian pathology
- CT scan: gold standard, shows free air and site of perforation
- Possible AXR and eCXR

What would you see on an AXR and eCXR with a GI perforation?
AXR
- Rigler sign
- Psoas sign (loss of the sharp delineation of the psoas muscle border due to fluid in the retroperitoneum)
eCXR (only 70% sensitivity so use CT)
- Cupola sign (look under right diaphragm)
- Pneumomediastinum or widened mediastinum if thoracic perforation

How are GI perforations managed?
Initially: broad spectrum abx, NBM, NG tube, IV fluid support, analgesia
Surgical:
- Identify underlying cause
- Repair underlying cause (omental/Graham patch for peptic ulcer or Hartmann’s procedure for perforated diverticular)
- Thorough washout
Conservative:
- Initial treatment if:
- elderly with comorbidities unlikely to survive surgery
- if sealed upper GI perforation on CT scan with no generalised peritonism
- localised diverticular abscess / perforation (<5cm) with only localised peritonitis and tenderness, and no evidence of generalised contamination on CT imaging

What are the surgical incisions needed to gain access to the following perforations:
- Stomach/duodenal
- Small bowel
- Large bowel
- Stomach/duodenum: upper midline incision with omental patch (Graham’s) and take a biopsy for malignancy
- Small bowel: midline laparotomy, oversew if bowel is viable, if not resect and anastomose or stoma
- Large bowel: midline laparotomy, do not anastomose if faecal content just stoma

What questions in the history should you ask if a patient has melaena?
Colour and texture of the stool– jet black, tar-like, and sticky
Associated symptoms – including haematemesis, abdominal pain, or a history of dyspepsia, dysphasia or odynophagia
PMH – including smoking and alcohol status, and inflammatory bowel disease
DHx– use of steroids, NSAIDs, anticoagulants, or iron tablets
ALWAYS DO DRE TO CONFIRM AND ABDOMINAL EXAM TO LOOK FOR EPIGASTRIC TENDERNESS, HEPATOMEGALY OR STIGMATA OF LIVER DISEASE

How is malaena managed?
- A to E approach to stabilise
- OGD once stable and resuscitated
- Tranfuse blood products if haemodynamically unstable or with a low Hb (<70g/L).
- Correct any deranged coagulation as, use reversal agents if patient on anti-coagulants or FFP +/- platelets with impaired liver function

What are some causes of rectal bleeding?
- If haemodynamically unstable then suspect upper GI bleed until proven otherwise
- Diverticular disease
- Ischaemic or infective colitis
- Haemorrhoids
- Malignancy (ALWAYS SUSPECT)
- Angiodysplasia
- Crohn’s disease or Ulcerative colitis
- Radiation proctitis.

What are some risk factors for adverse outcomes from acute rectal bleeding?

What are some of the causes of jaundice?

High levels of bilirubin (breakdown product of haem that is conjugated in the liver)

- Prehepatic: excessive breakdown of RBC
- Hepatic: dysfunction of hepatic cells so mixture of conjugated/unconjugated
- Post-hepatic: obstruction of biliary drainage
What is bilirubinuria?
Dark coca cola coloured urine when there is lots of conjugated bilirubin so either hepatic or post hepatic cause. Also pale stools
If normal colour urine likely pre-hepatic jaundice as unconjugated

What labatory investigations can be done if a patient presents with jaundice?
- LFTs
- Coagulation studies (PT is marker of liver synthesis function)
- FBC (anaemia, raised MCV, and thrombocytopenia all seen in liver disease) and U’s and E’s
- Liver screen

What is a liver screen?
Performed on patients where there is whereby there is no initial cause for liver dysfunction

How is jaundice managed?
- Treat underlying cause e.g ERCP if gallstone causing obstructive jaundice
- To treat itching give antihistamines or cholestyramine if obstructive jaundice
- Monitor for coagulopathy, treating promptly (either vitamin K or FFP)
- Oral glucose for hypoglycaemia
- If confused due to decompensating liver disease (hepatic encephalopathy) give laxatives (lactulose or senna) +/- neomycin or rifaximin to reduce the number of ammonia-producing bacteria

How do you do a hernia examination?
- Introduction: wash hands, gain consent, introduce, chaperone
- Inspect: get them to stand and look for asymmetry, scars, skin changes, lumps. Ask them to cough to protrude hernia
- Palpate: decide if scrotal (can get above) or groin swelling, decide if femoral or inguinal, ask patient to lie down and if reduces it is likely hernia, cough impulse.
Examine other side as often bilateral
- Complete: say you would assess genitalia for lymph nodes and any hernia into the scrotum.

How do you decide whether a hernia is femoral, direct inguinal or indirect inguinal?
- Above and medial pubic tubercle = inguinal hernia
- Below and lateral pubic tubercle = femoral hernia

How do you do a stoma examination?

Introduction: usual, put patient at 45 degrees, ask about any pain or output issues with stoma
Inspection: ask to remove stoma bag, inspect stoma, look for any complications like parastomal hernia (common with colostomies), prolapse, retraction, or infarction (black). Check skin for any erythema, ulceration or fistulas
Palpate: feel around stoma for any tenderness, ask patient to cough and see if cough impulse for parastomal hernia, digitate the stoma to assess for any stenosis and check patency

How do you do a digital rectal examination?

Introduction: usual, ask if any pain and tell them if any pain you can stop, chaperone
Preparation: position on their left side and bring their knees to their chest, positioning the buttocks at the edge of the couch, chaperone at their front side. get adequate lighting
Inspection: part buttocks and inspect perianal area e.g haemorrhoids, rectal prolapse, pilonidal sinus, skin disease
Palpation: (see image)
Complete: clean patient with towel, wash hands, offer to perform abdominal exam, clockface findings

What are some causes of acute epigastric pain?
- Perforated stomach ulcer
- Gastritis
- Pancreatitis
- Gallbladder pathology
- MI
- Pneumoa
- Oesophagitis (also retrosternal pain)
Ask about pain distribution, onset, character, timing, exacerbating factors, severity and radiation to work out cause of the epigastric pain

Once you have characterised acute epigastric pain with SOCRATES, what are some questions to ask in the history?

What is Boerhaave syndrome?
Spontaenous rupture of the oesophagus that presents with Mackler’s triad (vomiting, chest pain, subcutaneous emphysema)

What is the difference between acute and chronic pancreatitis?
- Acute pancreatitis is a life threatening inflammatory process. Usually due to gall stones or binge drinking
- Chronic pancreatitis develops insidiously over a long period of time and is characterised by progressive fibrosis and destruction of endo and exocrine glands. Usually due to chronic alcohol ingestion

What is the difference between a loop and end stoma?
Loop: used in emergencies and is only temporary, a loop of bowel is held out and held by an external device, two openings are made one for stool and one for mucus
End: stoma created from one end of the bowel, the other portion of bowel is either removed or sewn shut

When is it necessary to form a stoma?
1. Part of the colon has been removed so faeces can no longer pass through the anus e.g colon cancer, diverticulitis
2. A part of the colon has been operated on and needs to rest and heal, temporary
3. Faecal incontinence that is not responsive to other treatments

What are the differences between an ileostomy and a colostomy?
- Ileostomy is small bowel and is spouted and in the RIF. Often liquid that comes out
- Colostomy is large bowel, adhered to skin, can be anywhere on the abdomen and stool is solid

What is a Hartmann’s procedure?
Surgical resection of the rectosigmoid colon with closure of the rectal stump and formation of an end colostomy with a stoma bag
Done as a primary anastomosis is too risky at the time and may cause an anastomotic leak

How can you split the causes of PR bleeding into a surgical sieve and give some examples of causes?
Split anatomically

A patient presents to DASU with PR bleeding. An initial ABCDE assessment is done to check the patient is haemodynamically stable. What questions in the history should you ask about the bleeding?
- How much blood?
- How long has this been going on?
- Relationship of blood with stool?
- Any pain (usually painless) or prolapse when opening bowels?
- Any tenesmus (rectal cancer)?
- Any change in bowel habit?
- Any weight loss?
- Any symptoms of anaemia?
- Any drugs that could cause peptic ulcers?

What are Cushing’s and Curling’s tumours?
Cushing’s: gastric ulcer due to head injury, increased ICP causes vagal overactivity, prone to perforation
Curling’s: often seen in the stomach after intensive burns

How can you split the causes of an acute abdomen into a surgical sieve?

When a patient presents with an acute abdomen, apart from an abdominal examination what other examinations and investigations should you do?
- Groin
- PR
- PV/Scrotal

What is the difference between guarding and rigidity?
