Advanced True Learn #1 Flashcards
(789 cards)
An appropriate preoperative dose of oral midazolam is approximately what mg/kg in pediatric patients?
0.5 mg / kg
An appropriate preoperative pediatric dose of IV midazolam is what?
The dose of IV midazolam in pediatrics is 0.05-0.1 mg/kg.
What is the onset of action of oral midazolam?
The onset of action of oral midazolam is generally 15-30 minutes
How do you calculate a sodium deficit?
Ex: Sodium is 110 mEq/L and patient weights 100 kg.
Sodium deficit = (140 – serum sodium) * total body water
Total body water = kilograms of bodyweight * 0.6
In this patient, sodium deficit = (140 mEq/L – 110 mEq/L) * (100 kg x* 0.6) = 1800 mEq
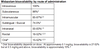
What hyponatremic patients should require hypertonic saline (3%)?
1. Symptomatic patients
- serum Na+ < 120 mEq/L
should have their serum osmolality corrected by 3% hypertonic saline (HS).
When should hypertonic saline be removed from hyponatremia treatment therapy?
Na+ rises > 120 mEq/L, remove hypertonic saline
What percent of the sodium deficit is correct in the first 24 hours with severe, symptomatic hyponatremia?
50% of the Na+ deficit is corrected during the first 24 hours
The rate of hypertonic saline administration should never exceed what?
The rate of hypertonic saline administration should never be higher than 100 mL/hr.
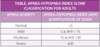
What is the difference in CRPS Type 1 vs 2?
Spontaneously arising pain is labeled CRPS type I
Whereas type II is associated with a prior nerve injury
What are the treatment options for CRPS?
Treatment consists of:
- Physical therapy (Gold Standard)
- Anticonvulsant medications (e.g. gabapentin)
- NMDA inhibitors (e.g. memantine)
- Sympathetic nerve blocks
- Spinal stimulators / intrathecal analgesic pumps.
What are the treatment options for Fibromyalgia?
The treatment of fibromyalgia
- Aimed at reducing pain
- Improving sleep, mood, and emotional balance.
- Physical therapy
- Analgesics (e.g., tramadol)
- Antidepressants (e.g., duloxetine)
- Anticonvulsants (e.g., pregabalin) have been shown to be beneficial for fibromyalgia.
What is the diagnostic criteria of myofascial pain syndrome?
Diagnosis a patient must demonstrate:
- Palpable, taut band
- Exquisite tenderness upon palpation of a nodule within the taut band
- Replication of the type of pain the patient reports with manipulation of the nodule and taut band
- Painful limitation to full passive range of motion of the particular muscle group.
What are the treatment options for myofascial pain syndrome?
Treatment
Local massage of the trigger points
Stretching of the muscle group
Local anesthetic injection into the trigger points
What are the 4 diagnostic subgroups of CRPS?
1) Sensory: hyperalgesia, allodynia
2) Vasomotor: temperature abnormalities or skin color changes
3) Sudomotor: fluid balance: abnormal sweating, edema
4) Motor: tremor, weakness, decreased range of motion
Sudomotor function refers to the autonomic nervous system control of sweat gland activity in response to various environmental and individual factors.
What is the [urine sodium] seen in SIADH?
Urine Sodium >20
Remember: Plasma is diluted and urine is concentrated
What is the [serum sodium] concentration in SIADH?
Low <135
What is seen in Cerebral salt wasting:
Na levels?
Intravascular volume?
Low Sodium
Low intravascular volume
How is Cerebral Salt Wasting Different from SIADH?
Same = Low Na, Increased [Urine Na]
Different: CSW is Hypovolemic, Increased UOP (Mechanism is excess secretion of Na and Water)
Different: SIADH is Normovolemic/Hypervolemic, Normal UOP
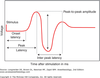
What is the mechansim of action of Clostridium Botulinum?
Flaccid neuroparalysis by preventing fusion and release of vesicles containing Acetylcholine at the Neuromuscular Junction

What is the mechanism of action of Clostridium Tetani?
Tetanus toxin from Clostridium tetani travels via neuronal retrograde transport up the motor neuron and enters the presynaptic terminal of inhibitory interneurons within the spinal cord.
Normal modulation of fine motor movement from descending motor pathways triggers the interneurons to exert their inhibitory effects via γ-aminobutyric acid (GABA) release.
The toxin prevents the release of GABA from the interneurons. Therefore, the inhibitory mechanism is inhibited and spastic neuroparalysis occurs.

Is Malignant Hyperthermia associated with Duchenne Muscular Dystrophy?
No
Complications like hyperkalemia and volatile anesthetic-induced rhabdomyolysis were once mistaken for malignant hyperthermia.
What cardiac conditions can arise from Duchenne muscular dystrophy?
1. CHF (#1 caause of death)
- Arrythmias (Aysrhythmias occur because of fibrosis in the cardiac conduction system and as a result of cardiomyopathies occurring with DMD. When under general anesthesia, these patients are at increased risk for dysrhythmias because of changes in the sympathetic and parasympathetic balance.
What medication should be avoided in DMD patients?
Succinylcholine & Volatile Anesthetics
(Upregulation of immature nicotinic receptors result in hyperkalemia and additional rhabdomyolysis can worsen potassium levels)
What are 3 alterations that should be known to the anesthesiologist regarding posterior fossa craniotomies?
- Venous Air Embolism
- Postural Hypotension
- Cardiac Alterations due to manipulation of brainstem