Exam 2 - Spring Flashcards
(171 cards)
spine is ___ shaped in utero and then what?
c-shared… then C and L become lordosis

TP of C1 is located…
behind the mastoid process of the skull
what has the largest cervical SP
C7 and then C2
fx of c-spine (3)
- protection
- exit for spin-N from cerv and brachial plexus
- mobility and support of head in environ
what is the keystone of the body
neck
what is major conduit of body?
c-spine b/w head and rest of body
superficial cervical fascia
b/w dermis and deep layer
N, bv, lymph
deep cerv fascia
3 layers: investing, pretracheal, prevert
supports viscera

posterior cerv M
nuchal line –> sacrum
- LBP can cause motion restriction to upper cervical region
sig mod of M at c2
- lots of oblique M txverse atlas and axis to occiput
cerv M act as…
“auto balancing system”
- keep head lvl during mvmt
- high concentration of proprio
- N reflexes to suboccitpal M
anterior cerv M
T3 –> occiput: mandible to hyoid, sternum, clavicle
- “strap M”
SCM
sup anterior M
imp for BALANCE
- high concentration of proprioceptors
fx:
- SB and R head in opposite direction
- bilateral flexor of c-spine
congenital torticollis
trapezius
superficial posterior M
- primary connection b/w head, neck, UE
nuchal line –> distal 1/3 of clavical and scapula
- elevates and retracts scapula
- extend, laterally flex, contralateral rotate head
levator scapulae
upper 4 c-vert –> medial border of scapula
fx: elev scapula
* lifting arm distributes forces to head
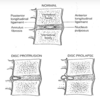
referred pain from acute herniated disc at mid c-spine lvl
scalene M
lateral stabilizers
- anterior and middle attached to rib 1
- posterior attaches to rib 2
- origin @ tubercles on C-TP
fx:
- flex c-spine
- breathing assist
restriction of OA or AA can cause restriction in what N?
vagus

cerv vasc
SC
- can be impinged by hypertonic scalene muscles or elevated 1st rib
carotid (anterior to c-vert)
- can listen for bruits
vert
- comes off SC
Vertebral Artery parth
C6 to TP of atlas –> Turns 90 degrees posteriorly –> Turns 90 degrees medially around the posterior edge atlas –> Turns to pass anteriorly and superiorly into the cranium where right and left vertebral a. form the basilar artery of the brain
what combo of mvmts on the c-spine causes the MOST structural challenge on vasc flow to brain?
extension, SB, rotation on SAME SIDE
- dixxiness
VERY impt to not put head into _____ during HVLA
extension
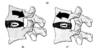
bony structure of c-vert
7 vert
vert foramina LARGEST at C1 and tapers down to C7 BUT vert become progressively LARGER
allow for sig mobility w/o restricting cord
Orientation of
Zygopophyseal (Facet) Joints
45 deg horizonal, face superior and posterior
b/w hori and coronal plane
STEEPER caudally (towards tail)
limits flex and extension

zygophyseal joints get more ________ more inferiorly
angle becomes flatter, more horizontal