Gene 500 Flashcards
(253 cards)
What are the 3 most common chromosomal abnormalities in recognized pregnancies?
1) Triploidy (100% SAB)
2) 45, X (99% SAB)
3) trisomy 16 (100% SAB)
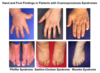
Large tongue, excess nuchal skin, auricular dysplasia, upslanting palpebral fissure, clinodactyly, hyperextensibility, single palmar crease, hypotonia
Down syndrome
47,XX,+21 (95%)
46,XX,rob(14:21) (4%)
Mosaic trisomy 21 (1%)
What are the complications of down syndrome?
Hearing problems (narrow ear canals)
Vision porblems
Cataracts, OSA
CHD
hypothyroidism
Leukemia
atlantoaxial instability
dementia
Small fingernails, short sternum, clenched hands (2 over 3, 5 over 4), micrognathia
Edwards Syndrome
Trisomy 18
- look for CHD, horshoe kidney, cerebllar hypoplasia, microphthalmia, central apnea
Sloped forehard, cutis aplasia, hypoterloirsm, cleft L/P, omphalocere, polydactyly, HPE
Patau, Trisomy 13
- Heart, CNS, renal, general anomalies
What are the most common karyotype findings for Turner Syndrome?
45,X - 50%
46, X, i(Xq) - 15%
45,X/46,XX mosiac - 15%
45X/46,X,i(Xq) - 5%
other
Low posterior hairline, renal anomalies, cardiovascular anomalies, short stature, edema in infancy
Turner Syndrome
+ gonadal dysgenesis, webbed neck, widely-spaced nipples
- Lack of secondary sex characteristics/ammenorhea in puberty
- Monitor for aortic root dilation
Hypogonadism, tall, gynecomastia, decreased muscle mass, osteopenia, low libido
Klinefelter
47 XXY (85%)
Mosaic 47XXY/46XY (15%)
- Increased risk for learning disabilities
What is the phenotype for 47XYY
Not dysmorphic
Tall, at risk for langage delay/low verbal IQ
- ~10-15 IQ points lower than siblings
What is 47XXX phenotype?
Tall, 70% have learning porblems
- no dysmorphic features
How is gonadal sex determined?
SRY -> SOX9
- established around 6 weeks gestation

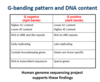
When does X inactivation occur?
2 weeks post-fertilization
What gene is expressed in the inactive X but not active X?
XIST
in Xq13
- produces large RNA molecules that coat inactive X
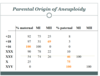
Which X is usually missing in 45X?
paternal 75%
Cystic hydroma, ovarian dysgenesis, low hairline, aortic root dilation
Turner Syndrome
Haploinsufficiency of PAR genes
- 2 Xs needed for ovarian development -> inactive X is reactivated in oogoina during meiosis (starts in fetal life)
When are patients witt Turner Syndrome at risk for gonadoblastoma?
When mosaic for 45X and 46XY and external genetalia is female or ambiguous
- okay if external genetalia is male
What does a ringed chromosome in turner syndrome mean?
Need to do FISH to determine if X or Y and if XIST is present
- if Y risk for gonadoblastoma
- if X and XIST is present -> PAR haploinsufficiency -> Turner
- if X and XIST is absent -> X disomy -> severe ID, OCD, dysmorhpic features, and congenital malformation
-
Xp21 deletion syndrome
DMD, RP, adrenal hypoplasia, ID, glycerol kinase
What does Xp duplication involving DAX1 do?
46XY females
- increased DAX1 dose can overcome sry
- w/ ID

In X-Autosome translocations, which X is inactivated?
If balanced; normal X nonrandomly inactivated
If unbalanced: abnormal X is nonrandomly inactivated

What is the reproductive consequence of X-autosome translocation?
Half of females infertile
All males infertile
Which chromosomes can be involved in robertsonian translocation?
Acrocentrics
13, 14, 15, 21, 22
What is the clinical consequence of balanced translocation?
Usually multiple miscarriages due to unbalanced offspring
- Phenotype depends on size, genes involved, monosomy vs trisomy
What type of segregation is most common in a quadrivalent?
Adjacent 1 (chromosomes next to each other with different centromeres go together)
- Alternate results in normal/balanced offspring