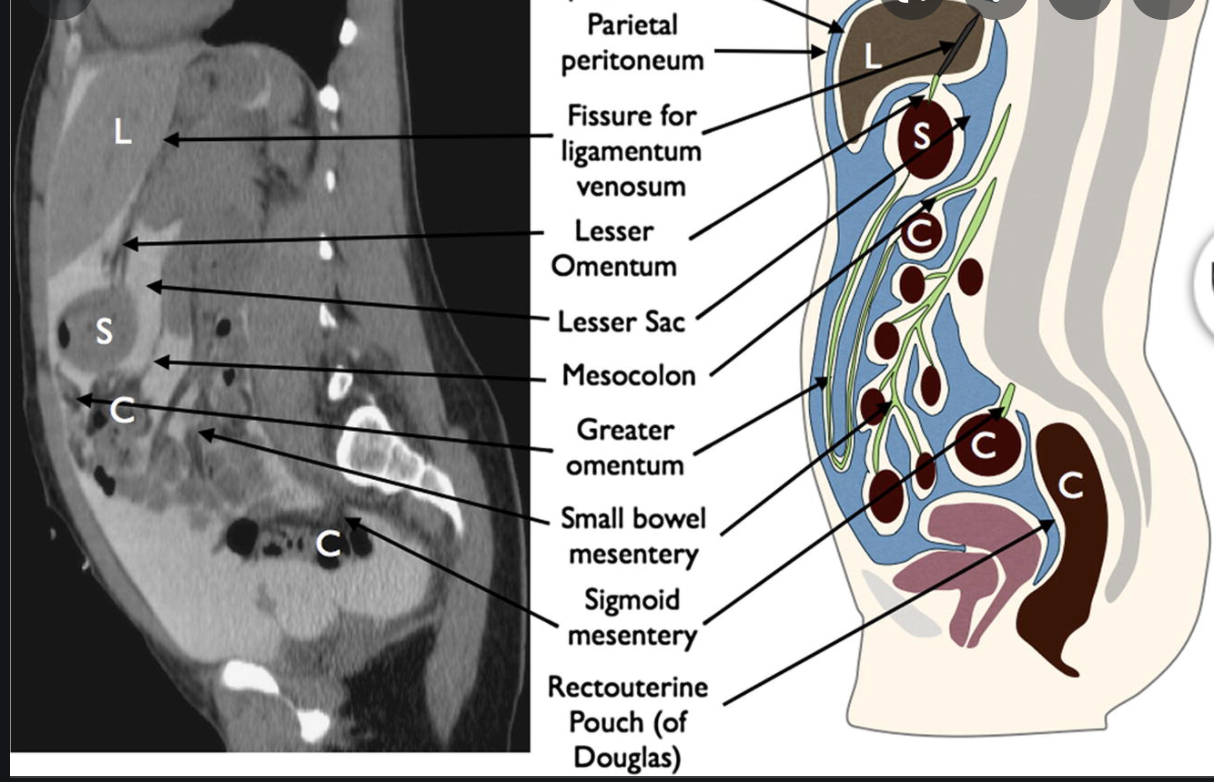
What are the Peritoneal spaces
- Subphrenic space
- divided by the falciform ligament into
- right subphrenic space between diaphragm nd liver
- left subphrenic space between diaphragm and spleen
- divided by the falciform ligament into
- Morison’s pouch
- right subhepatic recess
- hepatorenal recess
- most dependent portion of the abdominal cavity and collects fluid
- morisons pouch communicates with the
- lesser sac via the epiploic foramen
- subphrenic space
- right paracolic gutter
- Lesser Sac
- AKA Omental bursa
- posterior to the stomach and anterior to the pancreas
- medial superior extent between lesser curvature and left hepatic lobe, roofed by the gastrohepatic ligament
- access via the epiploic foramen/winslow
- Paracolic gutters
- pelvic
WHAT IS THIS?
histopathology
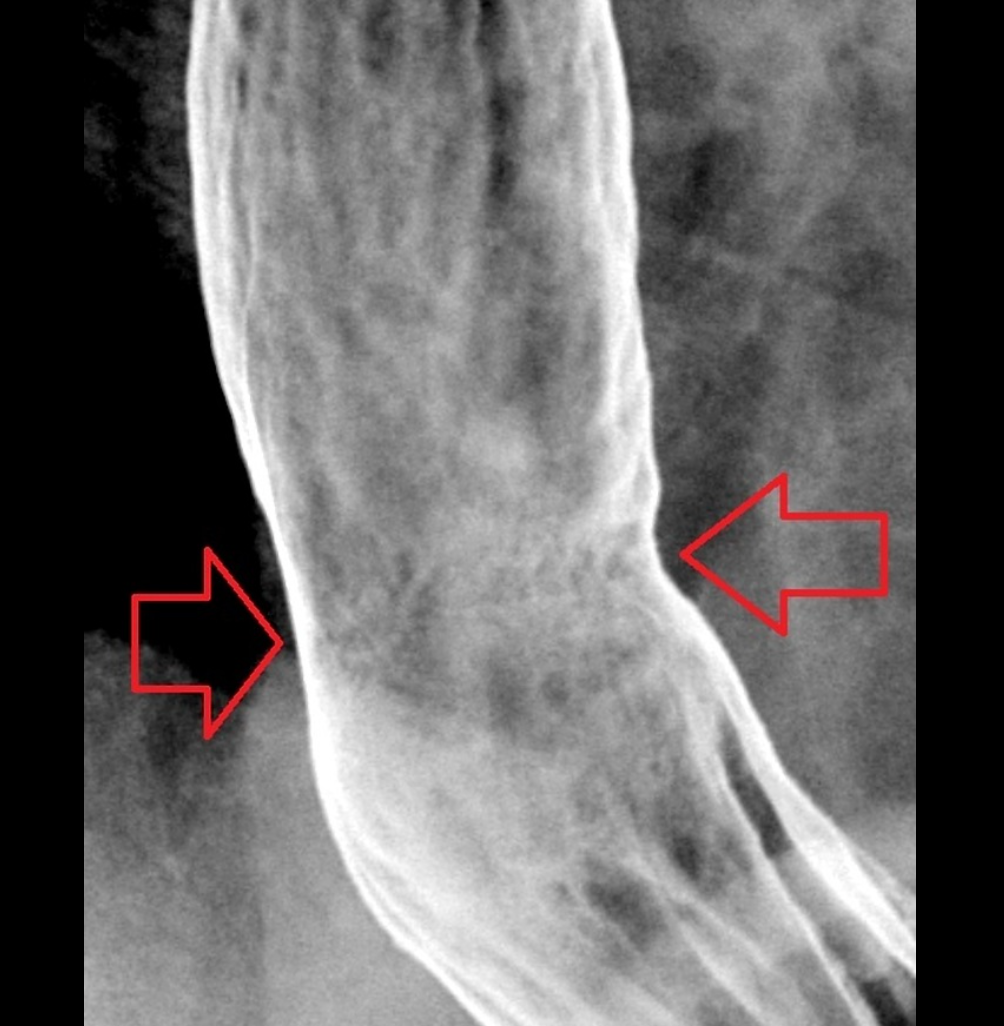
- Oesophagus is abnormally lined with columnar, metaplastic acid-secreting gastric mucosa.
- It is usually due to chronic reflux oesophagitis.
- Because there is an increased risk of oesophageal cancer, close follow-up and repeated biopsies are recommended
- IMAGING FEATURES
- A reticular mucosal pattern which may be discontinuous in the distal oesophagus (short segment) is the most sensitive finding.
- Suspect diagnosis if there is
- upper or midoesophageal stricture accompanied by reticular mucosal pattern below transition or ulcer
- Low strictures:
- the majority cannot be differentiated from simple reflux oesophagitis strictures and biopsies are required.
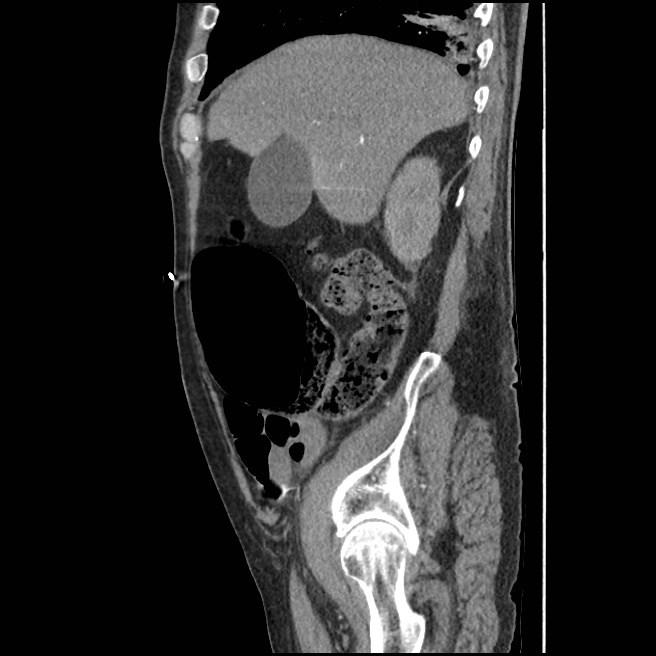
https://radiopaedia.org/cases/barrett-oesophagus?lang=gb
Zoomed-in images of the fine reticular pattern superimposed on oesophagitis (fine granular pattern) found in Barrett oesophagus. The area of fine reticulation is either circled in red or pointed to with red arrows.
Thanks to Steve Rubesin MD for this case.
Case Discussion
Biopsy proven Barrett oesophagus (no histologic dysplasia). This is more than an incidental finding on an oesophagram – this is a critical finding. By the time you find a lobulated oesophageal carcinoma it’s too late; the patient needs to be treated and followed at the first signs of metaplasia in the normal oesophageal stratified squamous epithelium.
It is important to get enough air/gas in the oesophagus in order to optimise one’s double contrast technique and pick up subtle findings like this. In addition to effervescent granules, it is often helpful to tell the patient to swallow as much air as possible while drinking the barium.
In this example, the Barrett oesophagus is at the gastro-oesophageal junction, but it can occur in patches anywhere from the mid-oesophagus down to the gastro-oesophageal junction.
DDx of calcified splenic foci on CT
8
- Healed granulomatous disease
- Sarcoid
- TB
- MAI
- Histoplasmosis
- PCP
- Candida
- Treated lymphoma
- Treated Mets
what is this?
who does it tend to occur in?
where does it tend to occur?
DDx?
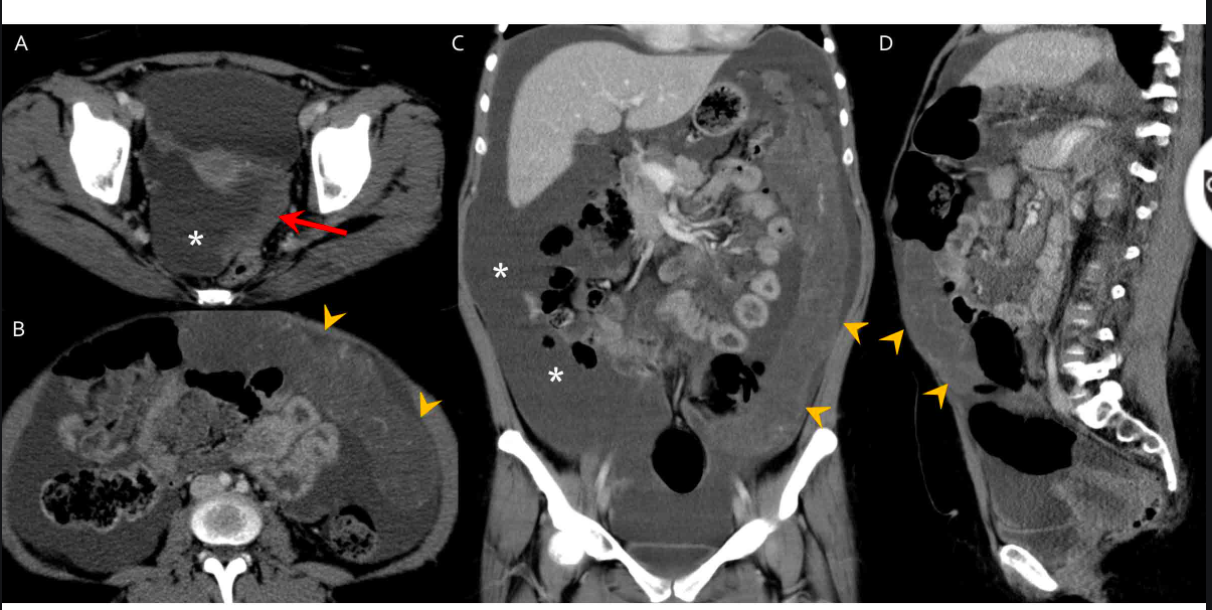
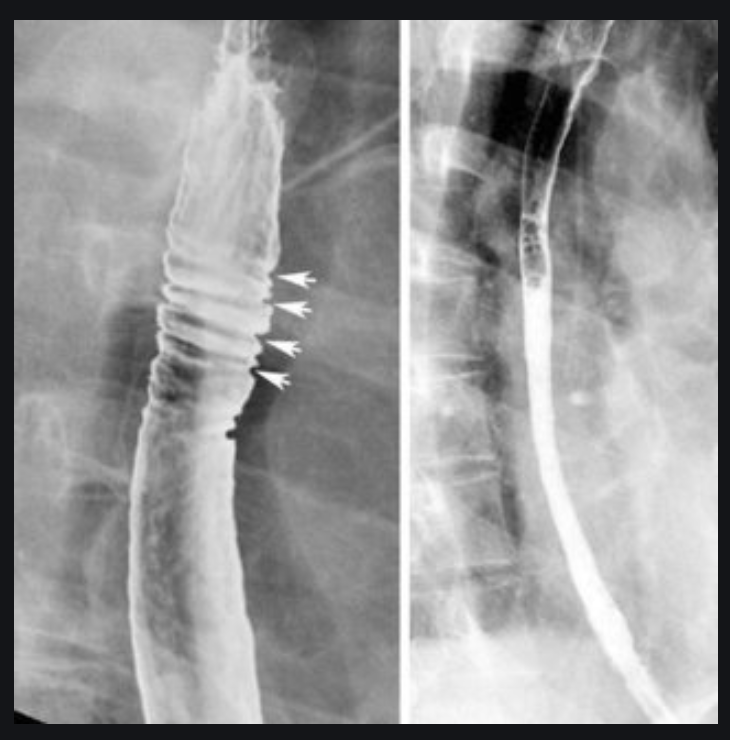
Desmoplastic small round cell tumor
- aggressive malignancy usually occurring in adolescents and young adults
- CT shows multiple peritoneal-based soft tissue masses with necrosis and hemorrhage.
- Hematogenous or serosal liver mets can be present without a detectable primary tumor
- Desmoplastic small round cell tumours of the peritoneum are a rare and highly aggressive primary peritoneal malignancy.
- Epidemiology
- Desmoplastic small round cell tumour is usually seen in young adolescents and have a male predominance with a mean survival of 2-3 years.
- Clinical presentation
- A desmoplastic small round cell tumour usually presents with a palpable abdominal mass and abdominal distension with discomfort.
- It is most commonly seen to arise from the pelvic peritoneal cavity, the retrovesical or rectouterine space being the most frequent locations. The tunica vaginalis of the testis is the next most common location.
- Solitary or multiple soft tissue masses are seen with no definite organ of origin, usually in the retrovesical or rectouterine space, which enhance heterogeneously on contrast studies. Necrosis, haemorrhage and fibrous components are common.
- Peritoneal seeding, lymph nodal involvement, liver and bone metastases are common modes of spread.
Differential diagnosis
- peritoneal carcinomatosis
- non-Hodgkin lymphoma
- malignant peritoneal mesothelioma
- rhabdomyosarcoma
- See also
- small round blue cell tumours
https://epos.myesr.org/posterimage/esr/ecr2018/143415/mediagallery/753353
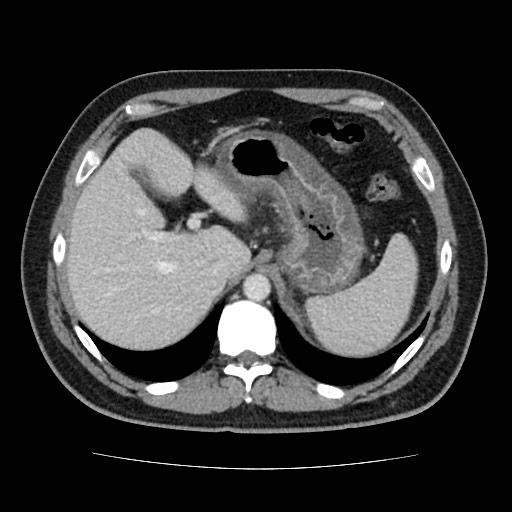
What is the Menetrier Disease Triad?
- Large gastric rugal folds (Hypertrophic gastritis), with protein-losing enteropathy.
- Clincial triad of
- Achlorhydria
- hypoproteinemia
- edema
- Typically occurs in middle aged men
- Complications
- gastric carcinoma 10%
- IMAGING FEATURES
- Giant gastric regal folds, usually the proximal half of the stomach
- Hypersecretion
- poor coating
- dilution of barium
- gastric wall thickening
- Small intestinal fold thickening bc of hypoproteinemia
- Peptic ulcers are common
- Case courtesy of Dr Michael P Hartung, Radiopaedia.org, rID: 83761
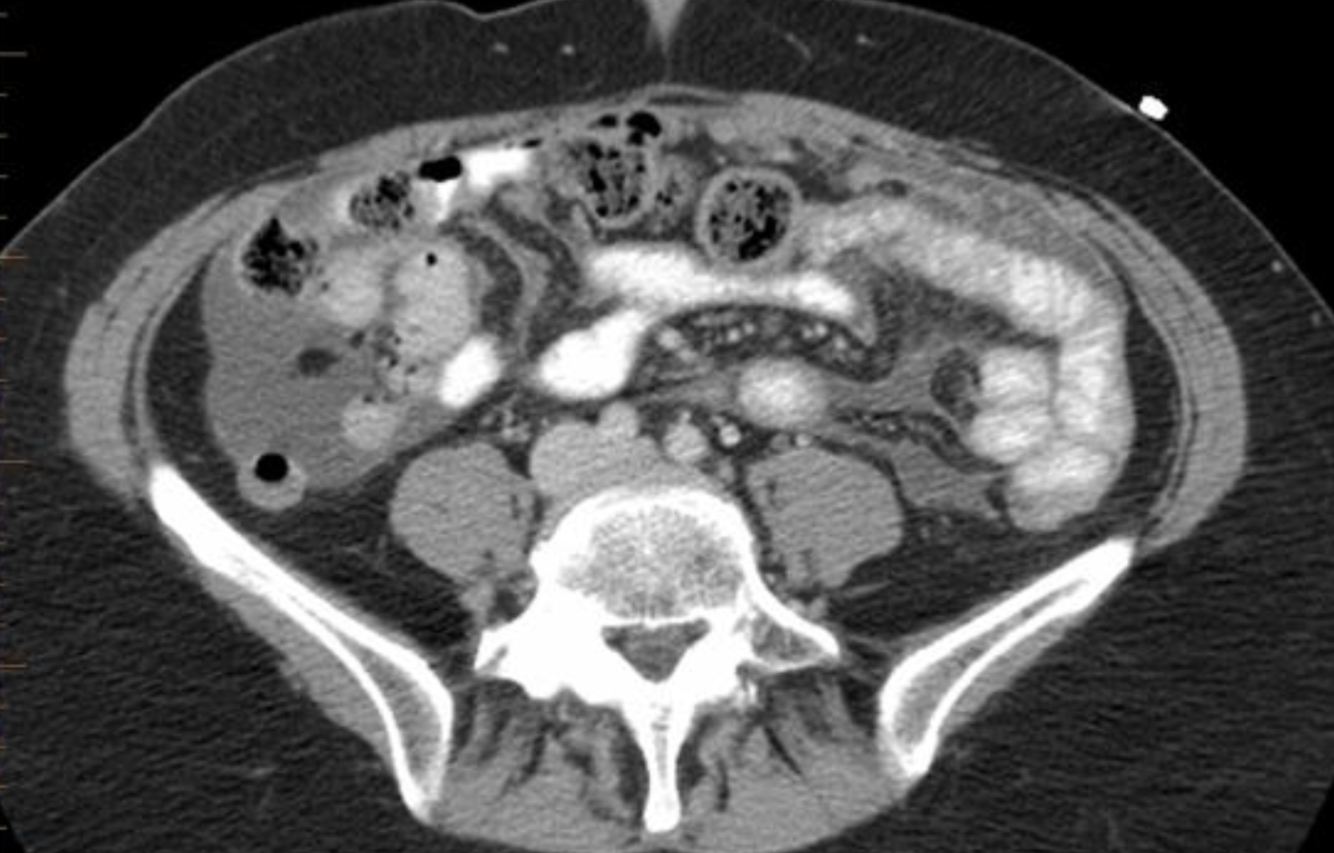
Gastric Polyps
- Incidence
- Types
- Incidence
- GPs are far less common than colonic polyps
- 2% of all patients with polyps
- Types
- Hyperplastic Polyps
- 80% of all gastric polyps
- <1cm
- Sessile
- Not premalignant
- A/w
- chronic atrophic gastritis
- Familial adenomatous polyposis (hyperplastic polyps in the stomach, adenomatous polyps in the colon
- typically similar size, multiple, and clustered in the fundus and body.
- Synchronous gastric carcinoma in 5-25% of patients.
- Adenomatous Polyps
- Infrequent
- malignant degeneration 50%
- solitary
- Villous polyps
- uncommon
- cauliflower like
- sessile
- Stong malignant potential
- hamartomatous polyps
- peutz-jeghers
- cronkhite-canada suyndrome
- juvenile polyposis
- Hyperplastic Polyps
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3992058/
What is this?
Caecal bascule
Dr Matt A. Morgan◉ and Assoc Prof Frank Gaillard◉◈ et al.
Caecal bascule is an uncommon type of caecal volvulus in which the caecum folds up over itself in an anteromedial orientation. In contrast to the more common forms of volvulus, there is no axial “twisting” component 4. A caecal bascule may occur in the setting of a large and mobile caecum and can result in closed obstruction involving the caecal pole and appendix.
Clinical presentation and treatment are not significantly different from the more common axial caecal volvulus.
Radiographic features
Plain radiograph
An abdominal radiograph of a patient with a caecal bascule will demonstrate a distended air-filled caecum located centrally within the abdomen. Occasionally the appendix is distended and air-filled, improving one’s confidence that the caecum is obstructed more distally.
Importantly, as the terminal ileum is usually not involved in the volvulus, the small bowel is not obstructed.
Cause of PUD?
- H pylori
- gram negative plays a major role in the development of a peptic ulcer
- Not all people with HP with develop ulcers
- Prevalence of HP: 10% <30yo, 60% of pop >60yo
- Prevalence of HP in DU and GU: 80-90%.
- Risk factor for adenocarcinoma and lymphoma.
- Approach
- precaution against infection should be taken by all GI personnel
- HP serology may become useful from the diagnosis of PUD.
- PUD heal faster with ABx and antacides then with antacids alone.
imaging features of SMA distribution ischaemic bowel disease
sick patients, hypotension, acidosis, high mortality
requeirses surgery, resection
Xray is similarly to SBO, may see pink-prints in SB wall
submucosal edema > pneumatosis > portal vein gas 5%
Symptoms of This?
Signs
Rx.
- Inflammatory eosinophilic esophagitis
- Dysphagia may be chronic, history of allergies, eosinophilia
- Segmental proximal or mid esophageal mild narrowing
- May involve the entire esophagus
- increased risk of iatrogenic tear
- Responds to steroids
What are the most common Peritoneal Metastases?
- Ovarian cancer
- GIT cancer
- Imaging features
- Greater omentum overlying SB “Omental Cake”
- masses on peritoneal surfaces
- Superior surface of sigmoid colon
- POD
- terminal ileum
- morison pouch
- Gastrocolic ligament
- malignant ascities
- May enhance with Gad as a result of increased permeability of peritoneum
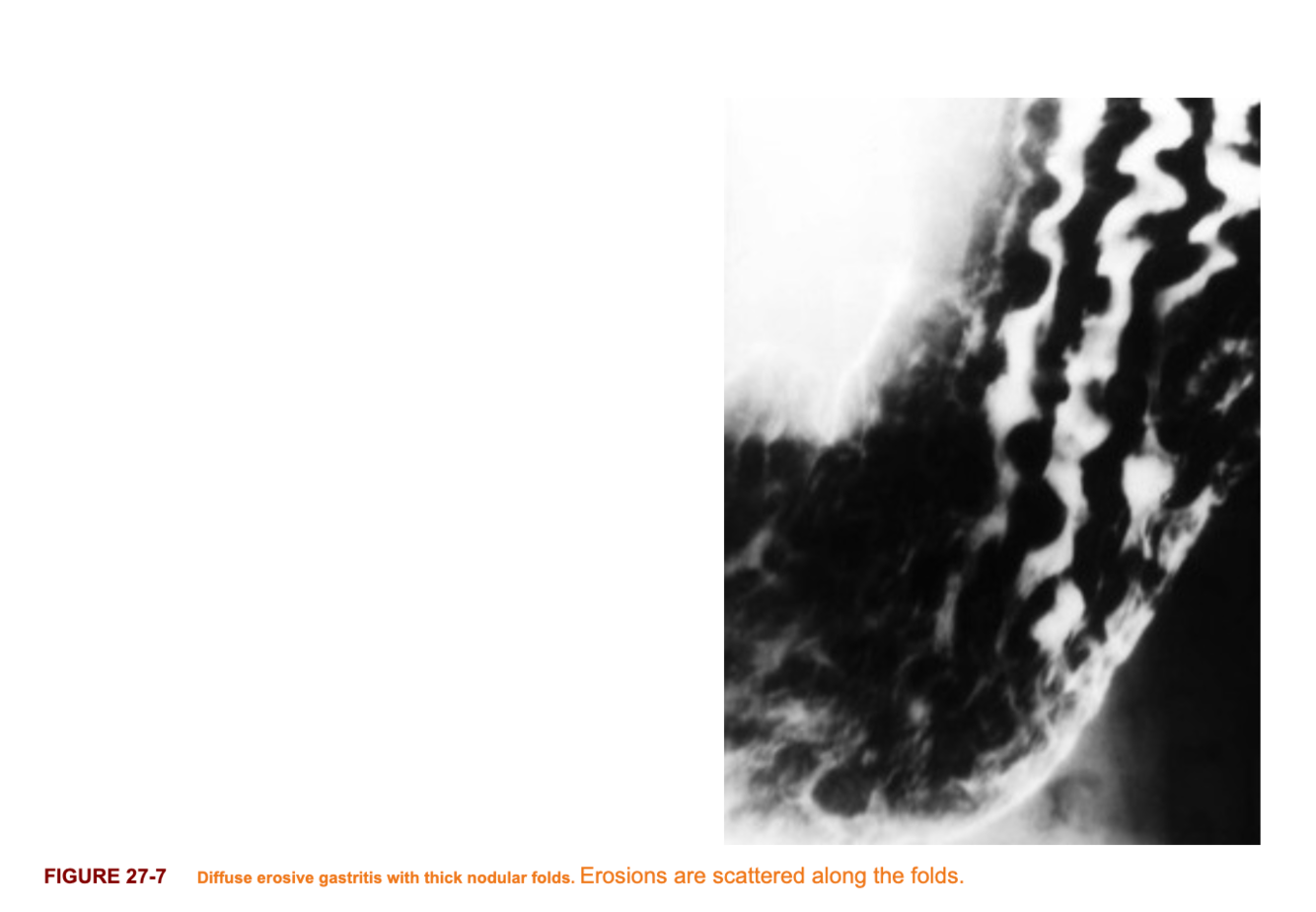
Imaging features of Gastritis
- Multiple tiny, apthoid like erosions throught the antrum and boy of the stomach
- Occurs on rugal folds
- Prominent area gastricae
what is the difference between an incarcerated and strangulated hernia?

- Incarceration
- a hernia that cannot be manually reduced
- strangulation
- occlusion of blood supply to the herniated bowel, leading to infarction
- Findings include bowel wall thickening, hemorrhage and pneumatosis as well as venous engorgement and mesenteric edema

Mesenteric panniculitis
- Case courtesy of Dr. Hani Makky Al Salam, Radiopaedia.org, rID: 10092
- A rare disorder characterized by chronic nonspecific inflammation involving the adipose tissue of the SB mesentery.
- When the predominant component is inflammatory or fatty, the disease is called mesenteric panniculitis.
- When fibrosis is the dominant component, the disease is called retractile mesenteritis.
- The latter is considered the final, more invasive stage of mesenteric panniculitis.
- The cause of this condition is unclear.
- Imaging features
- well-circumscribed, inhomogeneous fatty SB mesentery, displaying higher attenuation than normal retroperitoneal fat.
- The mass is usually directed toward the left abdomen where it extends from the mesenteric root to the jejunum.
- Spiculated soft tissue mass, a carcinoid mesenteric mass look-a-like.
What are 2 mimics of an ulcer
- ectopic pancreatic rests may contain a central umbilication that represents a rudimentary duct not ulcer. Commonly located in the antrum.
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6298353/
- Gastric diverticulum
- commonly in posterior fundus
- contains mucosal folds, neck
- changes shape during fluoroscopy.

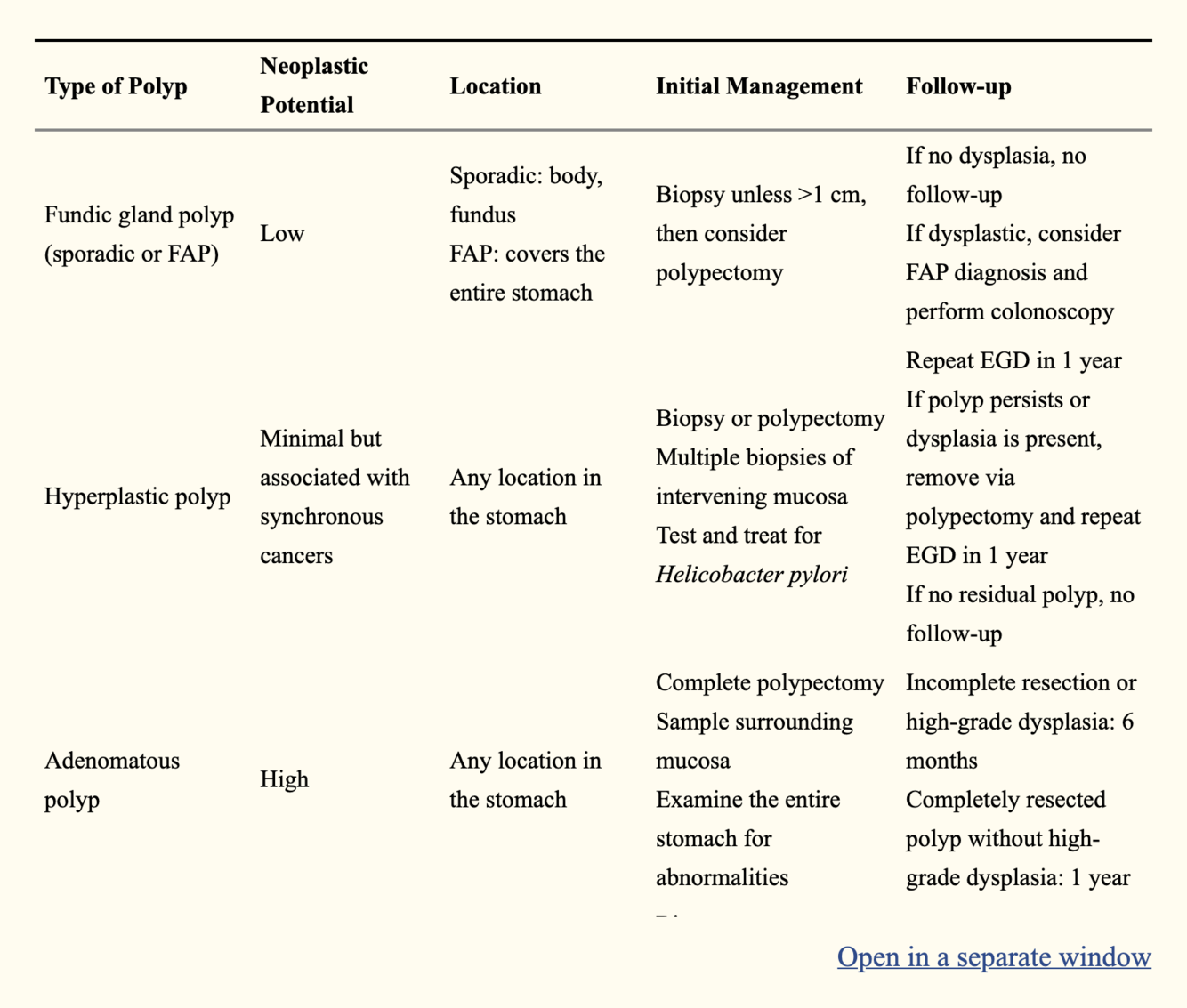
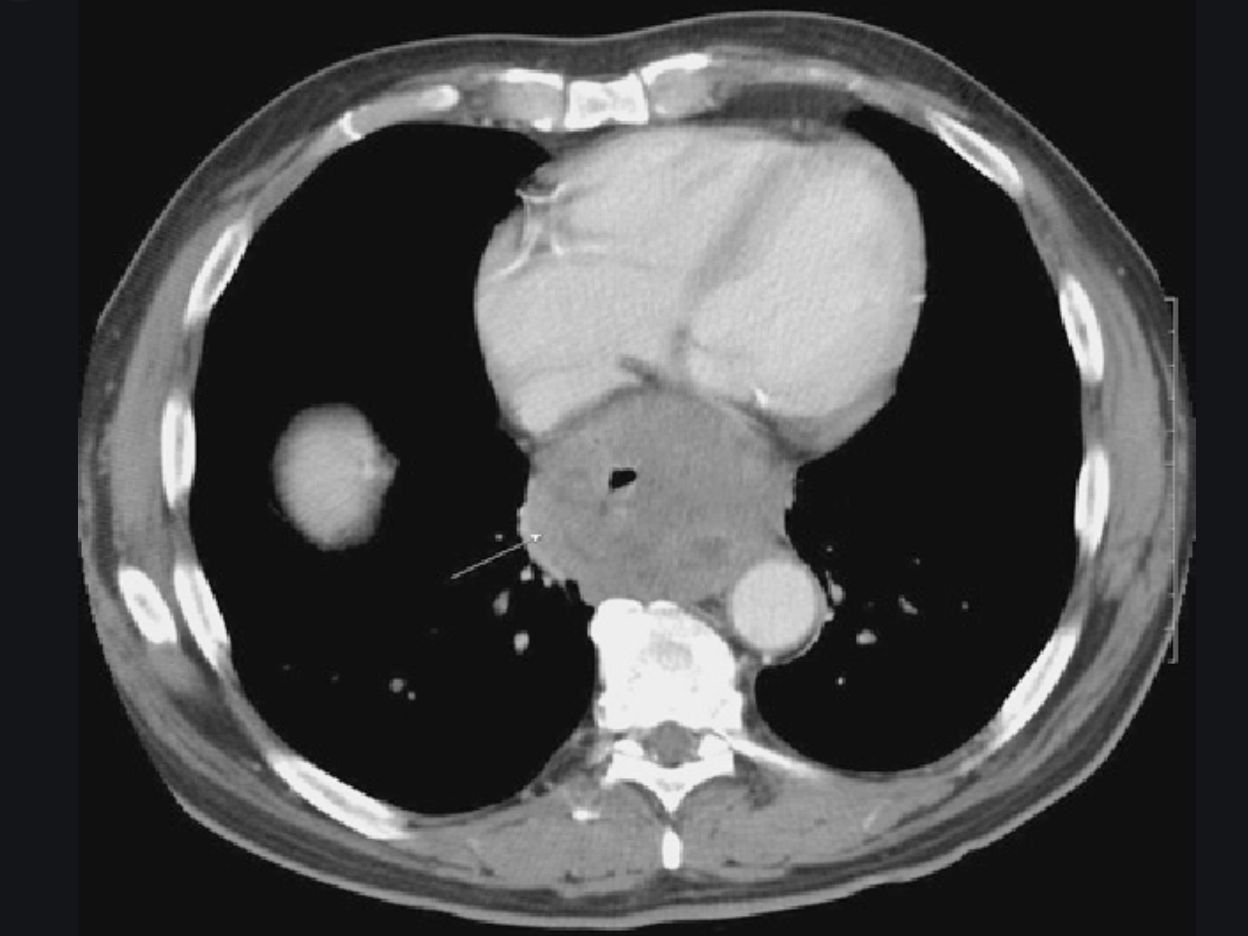
What is this?
What is a complication?

Epiphrenic diverticulum
- May occasionally be recognised on chest radiographs by presence of soft tissue mass.
- Often with an air-fluid level, that mimics a hiatal hernia
- Large diverticulum can compress the true oesophageal lumen, causing dysphagia.
Gastric carcinoma
- Fourth most common GI malignancy
- colon
- pancreas
- liver/bilary
- Stomach
- Risk factors
- pernicious anemia
- adenomatous polyps
- chronic atrophic gastritis
- Billroth II > Billroth I
- Location
- fundus/cardia 40%
- Antrum 30%
- Body 30%
- Staging
- T1:
- limited to mucosa, submucosa
- 5YS 50%
- T2
- Muscle, serosa involved
- 5YS 50%
- T3
- penetration through serosa
- T4
- Adjacent organs involved.
- T1:
- Imaging features
- Features of early gastric cancers
- Polypoid lesions Type 1
- > 0.5cm
- normal peristalsis does not pass through lesions
- difficult to detect radiographically
- Superficial Lesions, Type 2
- 2A <0.5CM
- 2B most difficult to diagnose (mucosal irregularity only).
- 2C 75% of all gastric ca.
- Folds tend to stop abruptly at lesion
- Excavated lesion, Type 3
- malignant ulcer.
- Polypoid lesions Type 1
- Features of early gastric cancers
causes?
Anatomy of this condition

- Causes
- anticoagulant tx
- femoral catheterisation
- trauma
- Appearance
- high-attenuation fluid collection
- first several days +/- fluid level (hc level)
- if there is no further bleeding the high-density RBCs decompose to reduced density fluid
- fluid-fluid level
- Anatomy
- usually confined to the rectus muscle
- About 2cm below the umbilicus (arcuate line), the posterior posterior portion of the rectus sheath disappears and fibers of all three lateral muscle groups (External oblique, internal oblique, and transversus abdominis) passes anterior to the rectus muscle.
- This arrangement has imaging significance in that rectus sheath hematomas above the line are confined within the rectus sheath
- Inferior to the arcuate line, they are directly opposed to the transversal fascia and can dissect across the midline or laterally into the flank (as seen in pic 2)
- Case courtesy of Dr Hani Makky Al Salam, Radiopaedia.org, rID: 9427

USS features of appendicitis
>6mm
noncompressible
>3mm wall thickness
shadowing appendicolith
echogenic periappendiceal fat
Oesophageal Lymphoma
- The oesophagus and stomach do not normally have lymphocytes, primary lymphoma is rare unless present from inflammation’
- secondary metastatic lymphoma is more common.
- Secondary oesophageal lymphoma accounts for <2% of all GIT lymphomas (Stomach > SB)
- Four radiographic presentations are:
- infiltrative
- ulcerating
- polypoid
- endoexophytic
What are the normal oesophageal contour deformities?
- Cricopharyngeus
- Postcricoid impressions (mucosal fold over vein)
- aortic impression
- LMB
- Left atrium
- Diaphragym
- Peristaltic waves
- Mucosa: thin transient transverse folds. Feline Oesophagus. Vs. Thick folds in chronic reflux oesophagitis. Tiny nodules in older adults: glycogenic acanthosis.
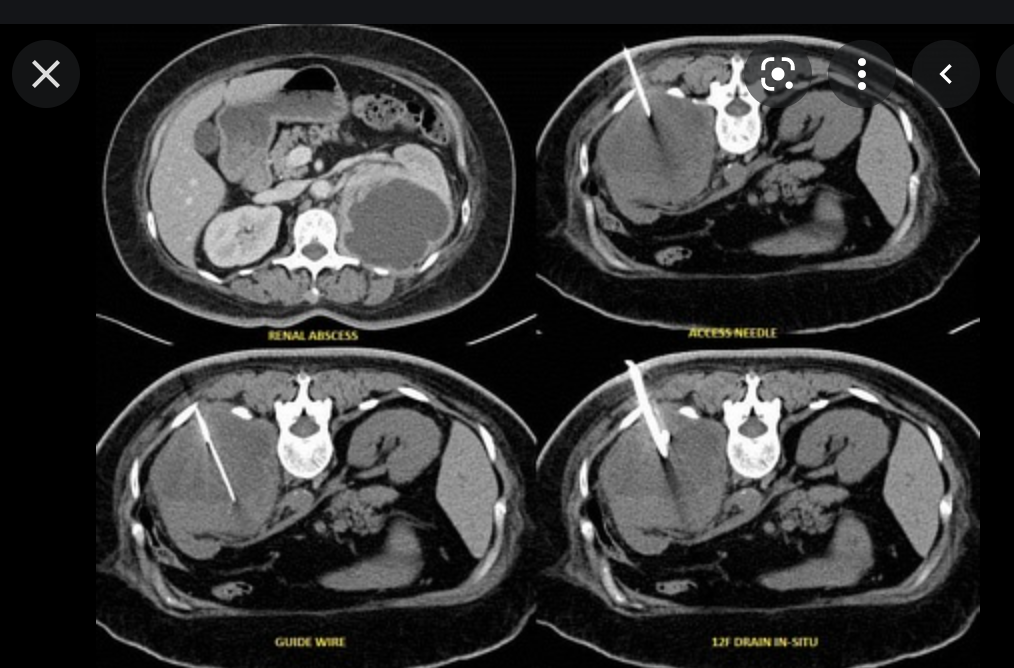
What are the two techniques used to percutaneous treat abdominal/pelvic collections
- Trocar technique
- commonly performed for large abscessers or collections with easy access.
- localise abscess by CT or US
- Anesthetize skin
- make skin nick and perforate subcut tissues
- place 8-16Fr abscess drainage catheter in tandem. Remove stylet
- Aspirate all fluid
- send for culture
- wash cavity with saline
- commonly performed for large abscessers or collections with easy access.
- Seldinger technique
- this is commonly performed for abscesses with difficult access or for necrotic tumours with hard rims
- localize abscess
- anesthetize skin
- localize abscess with 4, 6, or 8 inch seldinger or chiba needle (18gauge or 19gauge thin wall) under imaging guidance
- remove needle, leave outer sheath
- pass guide wire through sheath into abscess cavity
- dilate tract (8, 10, 12 Fn) over stiff guide wire
- Remove stiffener and guide wire.
- aspirate abscess
- this is commonly performed for abscesses with difficult access or for necrotic tumours with hard rims
What is this?
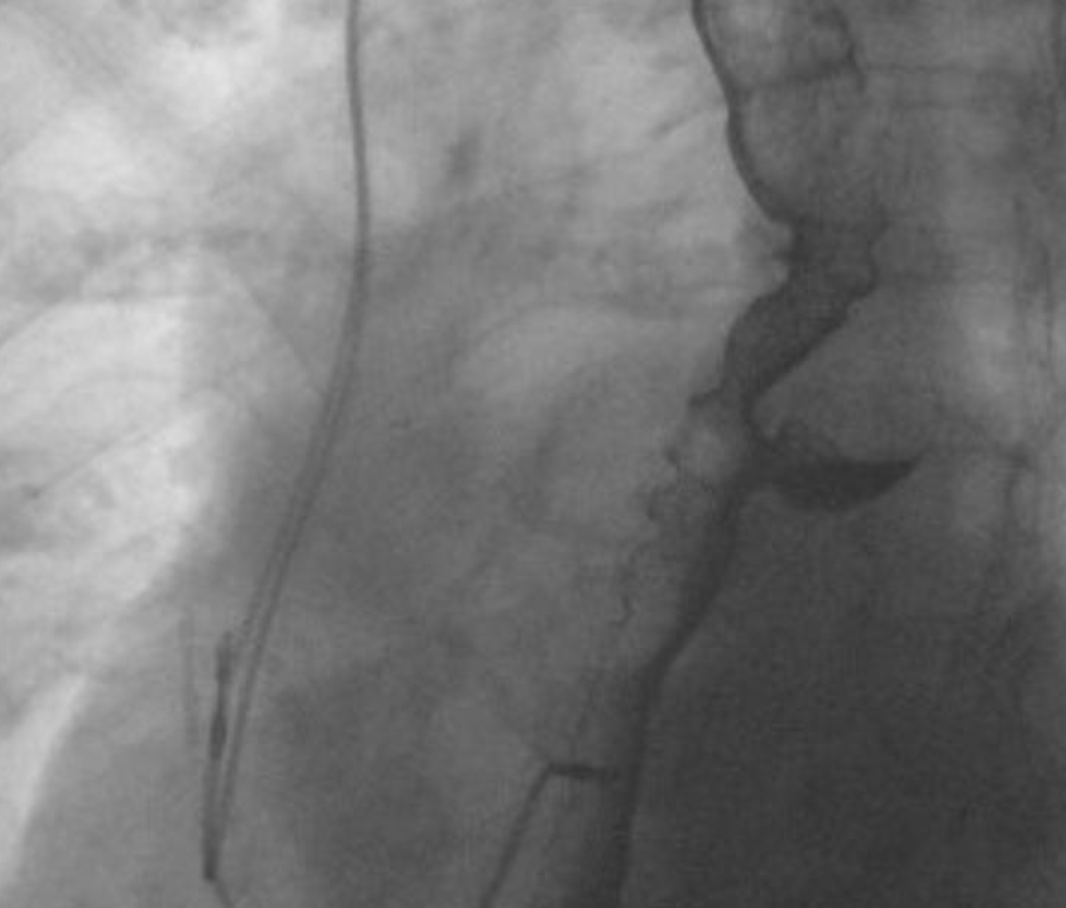
traction diverticula: are (true diverticula) which occur secondary to scarring, fibrosis and inflammatory processes (tuberculous adenitis) in the mediastinum pulling on the oesophageal wall
Complications of Gastric ulcers
- Obstruction
- posterior penetration of ulcer into pancreas
- perforation
- bleeding
- filling defect in the ulcer crater may present blood clots
- Gastroduodenal fistula
- double channel pylorus
























































-
CHEST IMAGING 1100
-
CHEST IMAGING 2100
-
CHEST IMAGING 343
-
CHEST IMAGING 4 (TUMOURS)81
-
CHEST IMAGING 5 PATHOLOGY2
-
CARDIAC IMAGING 1100
-
CARDIAC IMAGING 2100
-
CARDIAC IMAGING 3100
-
CARDIAC IMAGING 443
-
GIT 1101
-
GIT 2100
-
GIT 3100
-
GIT 4102
-
Hepatobilary155
-
Biliary System76
-
Pancreas66
-
Spleen24
-
Adrenal Glands70
-
GENITOURINARY IMAGING 197
-
GENITOURINARY IMAGING 2100
-
GENITOURINARY IMAGING 3100
-
GENITOURINARY IMAGING 4100
-
GENITOURINARY IMAGING 545
-
RETROPERITONEUM33
-
Male Pelvis10
-
GIT PATHOLOGY31
-
Skeletal Dysplasias18
-
MSK104
-
MSK Crack the Core70
-
MSK 295
-
MSK 3100
-
Neuro100
-
Neuro 222
-
NEURO 375
-
Head and Neck 1100
-
Head and Neck 2100
-
Head and Neck 3100
-
Head and Neck 4100
-
Head and Neck 555
-
DDX Head and Neck35
-
Vascular10
-
IR30
-
BREAST IMAGING52
-
OBSTETRICS17
-
GYNAECOLOGY40
-
PAEDIATRICS 196
-
PAEDIATRICS 297
-
PAEDIATRICS 395
-
Nuclear Medicine 134
-
PET CT16
-
Syndromes94
-
HAEMATOLOGY6
-
PATHOLOGY 141
-
Crack the core WHen I Say you say...489
-
Physics31
-
crack the core exam case companion18
-
EPONYMOUS Diseases/signs22
-
What the F&^# is that word?10
-
Radiology Signs25
-
Mnemonics36
-
GIT Pathology1
-
NEURO MRI PHYSICS14
-
GREAT CHEST XRAY CASES1
-
THIS PATIENT IS TYPICAL OF X CONDITION2
