Lecture 11- Control of blood pressure Flashcards
(78 cards)
Why is hypertension so dangerous?
Hard to notice
- Could be anyone of us… ‘the silent killer’- no symptoms until cardiovascular event
What is hypertension?
Sustained increase in BP
Ideal adult pressure is considered to be between
90/60 mmHg and 120/80 mmHg
how many stages of hypertension
3
- stage 1
- stage 2
- severe
stage 1 hypertension BP
>140/90 mmHg
stage 2 hypertension BP
160/100 mmHg
severe hypertension BP
>180 systolic or >110 diastolic
stage 1 is also called
pre-hypertension
What causes hypertension?
- In around 95% of cases the cause is unknown- ‘essential’ or primary (idiopathic) hypertension
- Where the cause can be defined it is referred as secondary hypertension
causes of secondary hypertension
- Renovascular disease
- Chronic renal disease
- Hyperaldosteronism
- Cushing’s syndrome
- Important to identify and treat the underlying cause
Why is it important to treat hypertension?
- Silent killer
- Although hypertension may be asymptomatic- it can have unseen damaging effects on
- Heart and vasculature
- Potentially leading to heart failure, MI, stroke, renal failure and retinopathy
HBP affects how many adults in england
1 in 4
how many hearts attacks and strokes are associated with high BP
at least half
also a major risk factor for chronic kidney disease, heart failure and dementia
Diseases attributable to hypertension- vascular diseases
- Stroke
- Heart failure
- Cerebral haemorrhage
- Chronic kidney failure
- Hypertensive encephalopathy
- Retinopathy
- Peripheral vascular disease
- Aortic aneurysm
- Left ventricular hypertrophy
- MI
- Coronary heart disease
how does hypertension lead to vascular diseases
increases both afterload and arterial damage
increased afterload can lead to
- left ventricular hypertropy –> heart failure
- increased myocardial oxygen demnad –> MI and ischaemia
arterial dmaage can cause ….. and ….. leading to :
atheroscleorsis and weakened vessels :
- MI
- Cerebrovascular disease stroke
- aneurysm
- nephorclerosis and renal failure
- retinopathy
how to examine targte organ damage/ clinical CVD
e. g. ask them anbout signs of ischaemia e.g. chest pain
e. g. feel for aneursysm
e. g. listen to peripheral pulses

left ventiruclar hypertrophy due to
increased afterload

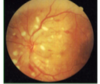
hypertensive retinopathy
- Hard parts- hard exudate (white parts)
- Red haemorrhages
atheroscelerosis
becomes heavilty calcified due to arterial damage

ischaemic stroke

chronic kidney disease
kidney reduces in size due to hypoxia

Effect of intervention
- Interventions show a significant reduction in mortality
- Any intervention which reduced blood pressure reduces all-cause mortality
- Every 10mmHg reduction in BP results in
- 17% reduction in CHD
- 27% reduction for stroke
- 28% reduction for heart failure
- 13% reduction in all-cause mortality








