Lecture 13- ECG changes during myocardial ischaemia Flashcards
(31 cards)
Coronary artery narrowing or occlusion lead to
ischemia or infarction (necrosis
changes in the ECG can be seen in
leads facing the affected area
Need to look at the P, QRS and T or all 12 leads
ischaemia
lack of oxygen to muscle but no muscle necrosis
myocardial infarction
muscle necrosis due to ischaemia
blood test markers in ischameia
will be negative for markers of myocyte necrosis (cardiac troponins)
blood test markers in MI
blood tests will be positive for cardiac troponins
STEMI
ST segment elevation MI
Non-STEMI
Non-ST segment elevation
Which ECG leads face which parts of the ventricles?
Inferior surface of ventricles
II, III and aVF
Which ECG leads face which parts of the ventricles?
Septum and anterior surface of ventricles
V1, V2, V3, V4
Which ECG leads face which parts of the ventricles?
Right ventricle and septum
V1 and V2 and aVR
Which ECG leads face which parts of the ventricles?
Apex and anterior surface of ventricles
V3 and V4
Which ECG leads face which parts of the ventricles?
Lateral surface of the ventricles
I, aVL, V5
ST segment elevation Myocardial infarction (STEMI) occurs due to
- Due to complete occlusion of coronary artery
- Full thickness of myocardium involved

ECG changes in STEMI
- Results in a positive deflection (going up)
- ST elevation is earliest sign of STEMI
- Indication for intervention

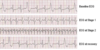
Evolving ECG changes in a STEMI

Why does myocardial necrosis and scar tissue from evolving and old infarcts leads to pathologic Q waves?
No electrical activity in dead tissue
No AP and no electrical current
ECG looks through dead tissue and picks up electrical forces from opposite side of infarcted heart
Are all Q waves pathologic
NOOOOOO
Small Q weaves represents normal left to right depolarised of the interventricular septum (typically seen in lateral leads- I, aVL, V5-6)
Deeper Q waves (>2mm) may be seen in leads III and aVR as normal variant (should not have any Q waves in lead V1-3)
Q wave is any negative deflection that precedes an R wave
Are all q waves a sign of an old infarct or depolarisation of septum?
- NO
- Pulmonary embolism may also lead to q waves in lead 3- part of the classic ECG findings for PE
- S wave in lead I
- Q wave in lead III
- Inverted T wave in lead III
Pathologic Q waves
- >1 small square wide (>40 ms)
- >2 small squares deep (mV)
- Except leads III and aVR- slightly bigger Q waves may be normal in these leads)

types of acute coronary syndrome
- stable angina
- unstable angina
- NSTEMI
- STEMI
stable angina
angina pain develops if there is an increased demand in the setting of a stable atherosclerotic plaque e.g. exercise
Vessel is unable to dialte enough to allow adequate blood flow to meet myocardial demand

unstable angina
plaque ruptures and a thrombus froms around the ruptures plaque causing aprtial occlusion of the vessel. Anginal pain occurs at rest or progresses rapdily over a short period of time